
Inadequate Coverage: An ACS CAN Examination of Short-Term
Health Plans
May 13, 2019
Executive Summary
Short-term, limited-duration health plans were originally intended to be a bridge when an individual had
a gap in comprehensive coverage – for instance when an individual was between jobs and temporarily
without access to an employer plan. Last year the Administration finalized a regulation that would
expand access to these products. Short-term plans traditionally have low premiums but fail to provide
the kind of comprehensive coverage an individual would need if they were diagnosed with a serious and
unplanned disease such as cancer. Issuers offering short-term plans are permitted to engage in medical
underwriting, meaning they can deny coverage to people with pre-existing conditions, can charge more
based on a person’s health status, or can refuse to cover services related to an individual’s pre-existing
conditions. They are also permitted to impose lifetime and annual limits on coverage and are not
required to provide coverage of the Affordable Care Act’s (ACA’s) essential health benefits.
To better understand whether short-term plans would be sold to cancer patients and, if so, what kind of
coverage a cancer patient could expect, we studied short-term plans in six states: Florida, Illinois,
Maine, Pennsylvania, Texas, and Wisconsin. We examined two zip codes within each of the six states to
better understand the extent to which premiums and deductibles varied between rural and urban areas.
Using a nationally-recognized online brokerage site, we created a hypothetical profile of an individual
57-year-old woman, non-smoker, looking for short-term, limited-duration plan availability in one urban
and one rural zip code in each of the six states. Our study assumed that the hypothetical woman would
be able to pass medical underwriting but then develop breast cancer once she was enrolled in the plan.
The goal was, in part, to understand how extensively a short-term plan might cover an unexpected and
costly condition that was not pre-existing and therefore not excluded outright. Some key findings are as
follows:
Pre-existing condition exclusions: We reviewed the brochures for each issuer examined in this white
paper and found that each one expressly stated that the plan excluded coverage for pre-existing
conditions. The final rule allowing for expansion of short-term plans requires this disclosure. Four of the
six brochures also included a “prudent layperson” standard within their definition of a pre-existing
condition. A prudent layperson standard includes undiagnosed conditions that produced symptoms
which would have caused a reasonably prudent person to seek diagnosis, care, or treatment. All
brochures said the issuer would consider as pre-existing only those conditions or symptoms that a
person experienced within a certain period of time prior to enrollment (i.e., two years or five years),
which is known as a lookback period. Depending on state law, some individuals can purchase back-to-

2
back, or “stacked” policies. Five of the six brochures examined expressly noted that any conditions
developed while covered under a previous plan were considered pre-existing under the new plan.
Premium variation: Generally speaking, plan premiums were higher for products with longer coverage
periods, with the exception being the 36-month plans offered in Pennsylvania. In a majority of the states
examined, average plan premiums were less expensive in rural areas compared to urban areas. We also
examined the number of plans offered in each geographic area and found robust issuer participation in
most geographic areas.
Hypothetical Patient Profile: Short-term plans can be marketed as a protection against unexpected
illness or injury. Given that most cancer diagnoses are unexpected we endeavored to assess what kind
of coverage an individual who was diagnosed with breast cancer after enrolling in a short-term plan
could potentially be offered. We used the example of a 57-year-old, non-smoking woman as a
hypothetical patient profile. The scenario assumed she would pass medical underwriting and be able to
purchase a short-term plan but would then developed breast cancer after enrollment. To keep the
scenario simple, we assumed certain issuers would not raise premiums or rescind coverage for the
sample patient, even though individuals diagnosed with cancer and covered under a short-term plan
would likely face either higher premiums or cancellation of coverage.
1
In our hypothetical, the total cost of treating breast cancer for the first year was estimated to be
$179,229.41, with health care costs highest in the month following diagnosis. We found the hypothetical
patient’s out-of-pocket costs would vary by duration of short-term plan as follows:
• 3-month plan: Assuming the enrollee was able to access all covered services in-network and
further assuming no delays in treatment, the plan would cover a little less than $60,000 in
services. The enrollee’s share of the treatment would amount to over $111,000, plus an
additional $363.90 in total premiums ($121.30 per month). The enrollee would become
ineligible for subsequent coverage of her cancer care in a short-term policy because her cancer
diagnosis would be considered a pre-existing condition.
• 6-month plan: Assuming the enrollee was able to access all covered services, the plan would
cover roughly $106,000 worth of the enrollee’s treatment. The enrollee would incur more than
$63,000 in cost-sharing related to her treatments, and an additional $1,570.56 in total
premiums ($261.76 per month).
• 12-month plan: The 12-month plan provided the most coverage relative to the other plans
examined. However, this plan still left the enrollee with over $40,000 in cost-sharing, not
including monthly premiums which totaled $31,184.52 ($2,598.78 per month). Taken together,
the enrollee’s cost-sharing and monthly premiums totaled $71,886.95, which is higher total
1
For example, people who are enrolled in short-term plans and then are treated for a serious illness may face
“post-claims underwriting,” in which the insurer examines their medical history and records for prior signs of the
condition, with the aim of deeming it pre-existing and avoiding payment of any related claims. Our scenario
assumed that did not happen to the enrollee. The scenario also assumed the insurer would pay the full in-network
charge of a given covered service, without any “balance billing,” which requires an enrollee to pay extra charges
not covered by the plan. For further details about the scenario used, see Appendix B.

3
cost-sharing than that provided under a 6-month plan.
In all cases examined, the individual incurred significantly higher out-of-pocket costs under her short-
term plan than had she purchased a plan on the marketplace, which provides more robust coverage of
services (including prescription drug coverage) and imposes a yearly cap on in-network cost-sharing of
$7,900. In addition, because the expiration of short-term coverage is not considered a qualifying event,
the individual would be unlikely eligible to enroll in ACA-compliant coverage until the next ACA open
enrollment period.
Lack of availability and clarity of plan documents: We discovered that it can be difficult – if not
impossible – for consumers to assess what services a short-term plan covers and does not cover prior to
purchasing coverage. Indeed, most of the details about plan coverage were included in the plan’s policy
documents, which were not made available to individuals shopping for coverage. This was particularly
true with respect to plan coverage of prescription drugs. While not all plans offered drug coverage,
those that did failed to provide any formulary information. Short-term plans also appeared to provide
limited coverage for preventive services.
2
Background
Having adequate and affordable health insurance coverage is a key determinant in surviving cancer.
Research from the American Cancer Society shows that uninsured Americans are less likely to get
screened for cancer and thus are more likely to have their cancer diagnosed at an advanced stage when
survival is less likely and the cost of care more expensive.
3
This not only impacts the nearly 1.8 million
Americans who will be diagnosed with cancer this year, but also the 15.5 million Americans living today
who have a history of cancer.
4
Short-term plans were originally intended to provide people who lacked health insurance coverage an
opportunity to obtain coverage as their name portends – for a brief period – before more
comprehensive coverage became available. These policies traditionally have low premiums but fail to
provide the kind of comprehensive coverage an individual undergoing active cancer treatment requires.
These plans were carved out from all federal health insurance laws, including the Affordable Care Act’s
2
For purposes of this study, we examined short-term plan issuers’ brochures to determine coverage of
prescription drugs, preventive services, and any other issues specifically related to cancer care. Other analysis has
shown that short-term plans also frequently do not provide coverage of maternity care or mental health and
substance use disorder. Pollitz K, Long M, Semanskee A, Kamal R. (2018, April 23). “Understanding short-term
limited duration health insurance.” Kaiser Family Foundation. Available at http://files.kff.org/attachment/Issue-
Brief-Understanding-Short-Term-Limited-Duration-Health-Insurance.
3
Ward E, Halpern M, Schrag N, Cokkinides V, DeSantis C, Bandi P, Stewart A, Jemal A. (2007). “Association of
Insurance with Cancer Care Utilization and Outcomes.” CA: A Cancer Journal for Clinicians 58(1), 9-31. Available at
http://www.cancer.org/cancer/news/report-links-health-insurance-status-with-cancer-care.
4
American Cancer Society. (2019). Cancer Facts & Figures 2019. Available at
https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-
figures/2019/cancer-facts-and-figures-2019.pdf.

4
(ACA’s) patient protections, and thus are permitted to engage in medical underwriting, meaning issuers
can deny coverage to people with pre-existing conditions, can charge more for coverage, or can refuse
to cover services related to an individual’s pre-existing conditions. These plans are also permitted to
impose limits on coverage and are not required to provide coverage of the ACA’s essential health
benefits.
5
Short-term plans are allowed to engage in post-claims underwriting, meaning that once a person is
enrolled in coverage if they submitted claims for an expensive service, the issuer would undertake an
investigation to determine whether the enrollee’s condition constituted a pre-existing condition. In
addition, short-term policies can and will end coverage at the policy’s term, even if the policyholder has
gotten sick and needs coverage to continue. Individuals whose coverage is rescinded or whose coverage
term ends are not generally eligible for a special enrollment period to enroll in comprehensive coverage
and thus are exposed to a gap in coverage.
In 2016, the Obama administration finalized a regulation that limited short-term plans to no more than
three months in duration (without the ability to extend coverage) and required such plans to display a
prominent disclaimer informing consumers that such coverage would not meet the ACA’s minimum
essential coverage requirements.
6
In doing so, the Obama Administration cited concerns that short-term
plans were being sold as primary coverage and were adversely impacting the ACA risk pools.
In 2018, the Department of Health and Human Services (HHS), Department of Treasury, and the
Department of Labor (DOL) finalized a rule that changed the previous policy, allowing for expanded
access to short-term plans.
7
Under the 2018 final rule, short-term plans were allowed to be sold for a
term of up to one year and be renewed, at the issuer’s discretion, for up to 36 months (without a
prohibition against the sale of back-to-back plans).
Some policymakers and advocates are concerned that the proliferation of short-term plans could
undermine the current insurance market by siphoning off younger, healthier individuals who would be
swayed by the lower premiums and would be more likely to pass medical underwriting compared to
older and sicker individuals. While older and sicker individuals could still seek coverage in the ACA-
compliant market, without younger and healthier individuals in the risk pool, the ACA-compliant market
would see premium increases to account for an older, sicker pool of enrollees. This effect is among the
5
The Affordable Care Act requires health plans to cover 10 Essential Health Benefits (EHBs): ambulatory patient
services; emergency services; hospitalizations; maternity care; mental health and substance use disorder services;
prescription drugs; laboratory services; habilitative and rehabilitative services; preventive and wellness services;
and pediatric oral and dental services.
6
Department of Health and Human Services, Department of the Treasury, and Department of Labor. Excepted
Benefits; Lifetime and Annual Limits; and Short-Term Limited-Duration Insurance. Final Rule. 81 Fed. Reg. 75316
(Oct. 31, 2016).
7
Department of Health and Human Services, Department of the Treasury, and Department of Labor. Short-Term,
Limited-Duration Insurance. Final Rule. 83 Fed. Reg. 38212 (Aug. 3, 2018).

5
reasons why a coalition of patient advocates and safety net health insurers have challenged the new
final rule in court.
8
The six states -- Florida, Illinois, Maine, Pennsylvania, Texas, and Wisconsin – and cities included in our
research were selected in order to provide for geographic diversity, varied overall size, and number of
expected cancer diagnoses in 2019. To date at least one state (Illinois) has enacted legislation to limit
the availability and duration of STLD policies.
9
Pre-Existing Conditions
Prior to the enactment of the Affordable Care Act (ACA), individuals who had a history of cancer were
often unable to purchase health insurance coverage on the individual market because plans could refuse
to cover an individual who had a pre-existing condition (such as cancer), charge higher premiums to an
individual with a pre-existing condition, and/or choose to cover the person with a pre-existing condition
but not cover services related to the pre-existing condition. Pre-existing conditions often included
serious diseases such as cancer but could also apply to more common conditions such as acne.
10
A survey conducted before these exclusions were prohibited in ACA-compliant plans found that 36 percent
of those who tried to purchase health insurance directly from an insurance company in the individual
insurance market were turned down, were charged more, or had a specific health problem excluded
from their coverage.
11
The Kaiser Family Foundation estimates that 27 percent of adult Americans under
the age of 65 have a “declinable” pre-existing condition,
12
with the prevalence of pre-existing conditions
increasing with age.
8
Litigation has been filed to halt the implementation of the short-term plan final rule. Association for Community
Affiliated Plans v. Treasury, No. 1:18-cv-02133 (D. D.C. filed Oct. 10, 2018). As of the date of this report that
litigation has not been resolved and is currently pending in the United States District Court for the District of
Columbia.
9
Goldberg, S. (2018, Nov. 28). “Illinois legislature overrides veto of short-term health plan limit.” Crain’s Chicago
Business. Available at https://www.chicagobusiness.com/health-care/illinois-legislature-overrides-veto-short-
term-health-plan-limit.
10
Schwab, R. (2016, Dec. 7). “From Acne to EcZema: The Return of Medical Underwriting Puts Millions at Risk for
Losing Coverage or Higher Premiums.” Georgetown University Health Policy Institute Center on Health Insurance
Reforms. Available at http://chirblog.org/from-acne-to-eczema-the-return-of-medical-underwriting-puts-millions-
at-risk-for-losing-coverage-or-higher-premiums/.
11
Doty M. M, Collins S. R, Nicholson J. L, and Rustgi S. D. (2009, July). “Failure to Protect: Why the Individual
Insurance Market is not a Viable Option for Most US Families.” Commonwealth Fund. Available at
https://www.commonwealthfund.org/sites/default/files/documents/___media_files_publications_issue_brief_20
09_jul_failure_to_protect_1300_doty_failure_to_protect_individual_ins_market_ib_v2.pdf.
12
Claxton G, Cox C, Damico A, Levitt L, Pollitz K. (2016, Dec.). “Pre-existing Conditions and Medical Underwriting in
the Individual Insurance Market Prior to the ACA.” Kaiser Family Foundation. Available at
http://files.kff.org/attachment/Issue-Brief-Pre-existing-Conditions-and-Medical-Underwriting-in-the-Individual-
Insurance-Market-Prior-to-the-ACA.

6
Because short-term plans are exempt from the ACA’s consumer protections, they are permitted to deny
coverage to individuals with pre-existing conditions. A summary of our analysis of issuer brochures is
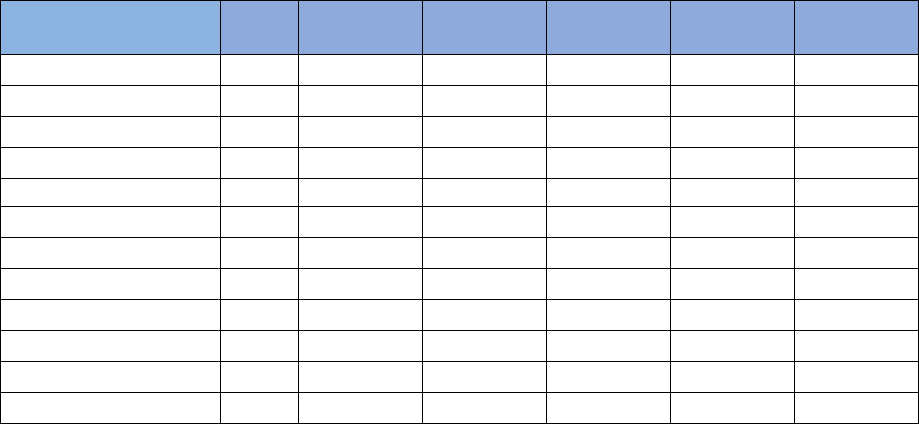
reflected in Table 1, below:
Table 1: Pre-Existing Condition Exclusions by Issuer
13
Issuer A Issuer B Issuer C Issuer D Issuer E Issuer F
Defined term No Yes Yes Yes Yes Yes
Includes prudent
layperson
standard
No Yes Yes Yes Yes No
Lookback period 60 months 60 months 12 months
60
months
24 months for
treatment
received;
12-month prudent
layperson
None listed
Pre-existing
condition
protections
extending to back-
to-back policies
No new
medical
questions
or waiting
periods for
stacked
coverage
Subsequent
policies are
subject to
new pre-
existing
condition
limitations
Subsequent
policies
only cover
conditions
covered
under a
previous
plan within
90 days
Unclear Subsequent
policies are subject
to new pre-
existing condition
limitations
Subsequent
policies are
subject to
new pre-
existing
condition
limitations
Based on author review of issuer brochures. In examining plan availability in the six states, we found six distinct issuers offering
coverage options.
* Issuer A’s brochure also noted that enrollees who purchased stacked policies would not be subject to additional medical
questions or new waiting periods.
“Pre-existing condition” definition: In reviewing the brochures for each issuer examined in this white
paper, we found that every issuer’s plan brochure expressly stated that coverage for pre-existing
conditions were excluded from coverage under the plan. All but one of the brochures we examined
defined the term “pre-existing condition,” though the definitions varied slightly.
13
Issuers are not identified by name because this paper includes a small illustrative sample of short-term plans;
and was not a comprehensive examination of all issuers in a state. Additionally, the report is not intended to
provide information about particular plans to consumers, but to discuss trends in the market.

7
Some of the issuer brochures we examined were intended for products sold in multiple states, and thus
contained state-specific terms that varied slightly from the general term used in the brochure.
14
Where
state variation existed it usually concerned the period under which an issuer could engage in post-claims
underwriting. One issuer’s brochure noted that the plan did not cover pre-existing conditions including
those not inquired about on the enrollment form. None of the brochures listed specific diseases or
conditions that would constitute a pre-existing condition for which the applicant would be denied
coverage.
“Prudent layperson” standard: Four of the six brochures also included a “prudent layperson” standard –
meaning that the issuer considers a pre-existing condition to be something that produced symptoms
which would have caused a reasonably prudent person to seek diagnosis, care, or treatment. The
“prudent layperson” standard provides issuers with additional flexibility to deny coverage to
applicants – or rescind coverage from individuals after they enroll. For example, after enrolling in a
short-term plan an individual is diagnosed with brain cancer. If upon investigation the issuer discovers
the individual experienced headaches prior to enrolling in the plan, the issuer may determine the brain
cancer is a pre-existing condition because a prudent layperson would have sought medical advice to
address their headaches and thus refuses to pay for the individual’s brain cancer treatments.
Lookback period: All issuer brochures examined noted they would employ a lookback period, which is a
limit on the amount of time, prior to enrollment, the issuer will look at a person’s medical history for
evidence of a pre-existing condition that warrants a denial of a person’s application or nonpayment of
the person’s claims related to the condition. The length of the lookback period varied by issuer. Five out
of the six brochures specifically noted the length of the look-back period.
Back-to-back policies: Depending on state law, short-term plans can now be “stacked”, meaning that an
individual could purchase back-to-back plans, thereby extending the period of time during which one is
enrolled in a short-term plan. Plan stacking is often confusing to consumers, who frequently assume that
issuers will not medically underwrite as long as the individual retains continuous coverage with the same
issuer. However, five of the issuers’ brochures expressly noted that any pre-existing conditions
developed while covered under a previous plan are considered pre-existing under the new plan. Thus, if
an individual developed a disease or condition while enrolled in a short-term plan offered by these
issuers, she would be unable to purchase another short-term plan because of the ability of plans to deny
coverage to individuals with pre-existing conditions. Because the expiration of short-term coverage is
not considered a qualifying event, the individual would be unlikely eligible to enroll in other coverage,
likely leaving her uninsured until the next open enrollment period.
The sixth issuer specifically highlighted the benefits of stacked plans by noting that while the cost-
sharing responsibilities would restart with a new plan, any medical conditions that arose while covered
under the initial short-term plan would be covered under the subsequent policy. But the brochure also
said these features were subject to plan limitations as noted in policy documents (which were
14
This could be confusing to consumers who would not only have to find information related to policy exclusions
among the general exclusions but would also have to look elsewhere in the document to determine if additional
exclusions or changes to the brochure were in effect depending on the state in which the applicant resides.

8
unavailable). On its face this statement suggests the issuer is providing an important consumer
protection. However, short-term plans can engage in post-claims underwriting, which would allow the
issuer to rescind coverage.
Premiums and Deductibles
Short-term plans typically have lower premiums relative to ACA-compliant health plans (particularly
unsubsidized ACA plans) because short-term plans are not required to provide comprehensive benefits
and can exclude individuals with pre-existing conditions or avoid covering their claims. We examined
two zip codes within each of the six study states to better understand the extent to which there was
premium variation. Health insurance premiums vary for a variety of reasons including, among other
things, the value of the benefits covered, health status of the enrollee, and geography. We were unable
to ascertain the actuarial value of covered benefits and the premiums listed do not account for any
medical underwriting.
15
The summary of our analysis is reflected in Table 2, below:
Table 2: Average Monthly Premiums for 57-Year-Old Woman in Chosen Zip Code by State
City State Urban/Rural 3-month 6-month 12-month 36-month
Chicago (60639) IL Urban
$349.29
$498.16
LaSalle (61301) IL Rural
$271.22
$384.80
Houston (77051) TX Urban
$492.84
$666.70
Mission (78572) TX Rural
$473.23
$646.61
Allagash (04774) ME Rural
$266.15
$393.86
Portland (04103) ME Urban
$266.15
$393.86
Jackson (32446) FL Rural
$311.26
$403.93
Miami-Dade (33172) FL Urban
$393.33
$506.18
Milwaukee (53202) WI Urban
$312.93
$398.65
Waupaca (54981) WI Rural
$272.38
$385.48
Pittsburgh (15286) PA Urban $290.48
$416.35
$576.75
$386.34
Towanda (18848) PA Rural $289.74
$393.79
$545.16
$344.65
Source: Analysis of premium provided by online broker. Averages include median premium across all issuers. Premiums do not
reflect medical underwriting, meaning actual premiums could be higher than shown here.
The 3-month and 36-month plan options were only available in Pennsylvania.
Coverage length: In only one state – Pennsylvania – 3-month and 36-month plans were available.
16
In all
of the states that we examined, 6-month and 12-month plans were available. Generally speaking, plan
premiums were higher for products with longer coverage periods. One notable exception was that
average plan premiums for the 36-month plans were less than premiums for 12-month plans. Average
15
In general, it was challenging to determine specific information regarding plan coverage and benefits, as
discussed further in the “Consumer Disclosure Material” section of this paper.
16
This could be due to the fact that the data for plan availability in Pennsylvania was gathered in March 2019,
rather than November 2018 when the information for the other states was gathered.

9
monthly premiums for 36-month plans in Pittsburgh, Pennsylvania were $190.41 less than the average
monthly premium for the 12-month plan and $30.01 less than the average monthly premiums for the 6-
month plan. Similarly, in Towanda, Pennsylvania average premiums for 36-month plans were $200.51
less than average premiums for 12-month plans and $49.14 less for 6-month plans.
Urban versus rural: In a majority of the states examined, premiums were on average less expensive in
rural areas compared to urban areas. The notable exception involved products offered in Maine which
had the same average premium for both urban and rural areas. Illinois and Florida saw the greatest
variation in average premiums between rural and urban areas.
In addition to analyzing the premiums of short-term health plans, we also examined the use of the
deductibles for these plans. Short-term plans, like most health insurance coverage, utilize a benefit
design that includes a deductible.
17
The summary of our analysis is reflected in Table 3, below:
Table 3: Most Common Deductibles by State
City State Urban v Rural 3-Month 6-Month 12-Month 36-Month
Chicago (60639) IL Urban
$5,000 $5,000
LaSalle (61301) IL Rural
$5,000 $5,000
Houston (77051) TX Urban
$5,000 $5,000
Mission (78572) TX Rural
$5,000 $5,000
Al
l
agash (04774)
ME
Rural
$10,000
$10,000
Portland (04103) ME Urban
$2,500 $2,500
Jackson (32446) FL Rural
$5,000 $5,000
Miami-Dade (33172) FL Urban
$5,000 $5,000
Milwaukee (53202) WI Urban
$5,000 $5,000
Waupaca (54981) WI Rural
$10,000 $5,000
Pittsburgh (15286) PA Urban $10,000 $10,000 $5,000 N/A
Towanda (18848) PA Rural $10,000 $5,000 $5,000 N/A
Source: Analysis of deductibles provided by online broker.
Some plans use a separate prescription drug deductible, to the extent they provided any drug coverage, which is not reflected
in the above data.
The 3-month and 36-month plan options were only available in Pennsylvania. Plan deductibles varied so significantly for the 36-
month plan options that it was not possible to ascertain the most commonly utilized deductible.
Deductibles: Every state examined offered 6-month and 12-month plan options, and the most widely
used deductible for both options was $5,000 – meaning that the enrollee would have to spend $5,000
before the plan began covering services. The most common deductible for the plans examined in
Allagash, Maine was the only area examined with an average deductible of $10,000 for both the 6-
month and 12-month plan options.
17
A deductible is the amount an individual pays out of pocket before their health plan starts to cover services.
10
Individuals who purchased back-to-back policies would have deductible obligations for each new period
of coverage. In other words, an individual who purchased four consecutive 3-month plans, would have
to meet a new deductible every three months before the plan would begin to cover services.
Plan deductibles varied widely, with every state having plans available with a deductible as low as
$1,000. In every state but Maine, plan deductibles were as high as $12,500. Plan deductibles in Maine
ranged from $1,000 to $10,000. As a point of comparison, plans sold on the ACA marketplace are
required to cap total annual out-of-pocket costs for in-network services at $7,900 and provide more
robust coverage (including prescription drug coverage).
Finally, we noted that plan availability was relatively robust in each geographic area we examined. The
summary of our analysis is included in Table 4, below:
Table 4: Plan Options and Number of Issuers by State
City
State 3-Month 6-Month 12-Month 36-Month
Number of
Issuers
Chicago (60639) IL 42 45 5
LaSalle (61301) IL 42 45 5
Houston (77051) TX 42 50 5
Mission (78572) TX 42 50 5
Allagash (04774)
ME
16
16
1
Portland (04103) ME 16 16 1
Jackson (32446) FL 42 50 5
Miami-Dade (33172) FL 42 50 5
Milwaukee (53202) WI 36 46 4
Waupaca (54981) WI 41 44 4
Pittsburgh (15286) PA 26 19 20 4 5
Towanda (18848) PA 26 19 20 4 5
Source: Analysis of information provided by online broker.
Plan options: Every state we examined had robust issuer participation, with the two geographic areas in
Maine (Allagash and Portland) having the fewest plan options – only 16 plan choices for both the 6-
month and 12-month plan options. The two geographic areas in Texas (Houston and Mission) offered
the most robust plan choices with a total of 92 plan options (between both the 6-month and 12-month
plans) in each of the geographic areas.
As discussed in more detail in the Consumer Disclosure section below, consumers shopping for coverage
were provided with basic information about the plan (premium, deductible, coinsurance), but we were
not able to ascertain the actuarial value of the covered benefits. Thus, it would be challenging for a
consumer to make an informed decision when choosing a plan.
Issuer participation: None of the geographic areas examined provided plan options from all six issuers
examined in this report. Most geographic areas – those in Illinois, Texas, Florida, and Pennsylvania –

11
included plan options from five out of the six issuers examined in the report. Maine was the only state
examined that only had one issuer.
Interestingly, in four of the six states examined, one issuer appeared to offer mirror plans. For example,
in looking at the index of plan choices in Jackson, Florida this issuer offered a 12-month plan with a
monthly premium of $329.41, a $10,000 deductible, and 20 percent co-insurance on covered services. In
the index of plans, the immediately subsequent plan offering was an identical plan, with the same
coverage period, premium, deductible, and cost-sharing. Since this issuer used a standard brochure
across all plans, it was impossible to ascertain what, if any, difference existed between these two plan
offerings. This duplication of plans appeared in more than one geographic area and often several times
per area, which suggested it was a conscious decision by the issuer rather than an error on the part of
the online brokerage site.
Cancer Care Illustrative Examples
Short-term plans are not subject to the patient protections provided under the ACA. As noted, they do
not have to offer coverage of essential health benefits and these plans can deny coverage to individuals
with pre-existing conditions. Most individuals with cancer (or a personal or family history of cancer)
would likely be denied coverage altogether due to the medical underwriting practice employed by these
issuers. For those able to pass medical underwriting and enroll in a short-term plan, cancer would likely
be treated as a pre-existing condition, and coverage for cancer treatment would be excluded under the
policy.
Some cancer patients are diagnosed with cancer after having no prior medical history or symptoms –
and therefore it is possible an individual could pass medical underwriting, be enrolled in a short-term
plan, and then be diagnosed with cancer. However, short-term plans have been known to rescind
coverage, claiming the enrollee had a pre-existing condition that was not adequately disclosed, when
faced with a large claim, such as those associated with cancer care.
18
We wanted to determine what coverage potentially could be provided to a woman who was diagnosed
with breast cancer after enrolling in a short-term plan, setting aside the other problems with short-term
plans that such a person would likely face in real-life. In 2017, the American Cancer Society Cancer
Action Network released The Cost of Cancer, a report focusing specifically on the costs of cancer borne
by patients in active treatment as well as survivors.
19
To more fully illustrate what cancer patients
actually pay for care the Cost of Cancer report also presents scenario models for a breast cancer patient.
For the purposes of this report, we used cost and utilization information from the Cost of Cancer
18
Levey, N. N. (2019, April 2). “Skimpy health plans touted by Trump bring back familiar woes for consumers.” LA
Times. Available at https://www.latimes.com/politics/la-na-pol-trump-shortterm-health-insurance-consumer-
problems-20190402-story.html.
19
American Cancer Society Cancer Action Network. (2017, April). The Costs of Cancer: Addressing Patient Costs.
Available at www.fightcancer.org/costsofcancer.

12
report,
20
and for purposes of the illustration assumed the plan covered all services unless otherwise
expressly noted in the plan brochures.
3-Month Plan
Three-month policies were only available in one of the states examined (Pennsylvania). Noting that
consumers often chose a health plan based on the premium offered, we chose to examine a three-
month plan with the lowest premium offered in Pittsburgh, Pennsylvania.
21
For this analysis, we assume
a new enrollee who was diagnosed with breast cancer at the beginning of the policy would not have her
policy rescinded.
This policy offered coverage for a 57-year old, non-smoking woman as follows:
Monthly Premium
Deductible
Coinsurance
Out
-
of
-
Pocket Limit
$121.30
$12,500
30%
$22,500
This particular plan operated an Exclusive Provider Organization (EPO) network, which required the
enrollee to use only in-network providers. For purposes of our analysis we assumed all providers were
in-network. The brochure noted that policies issued in Pennsylvania would require coverage of one
routine mammogram for individuals over 40 years of age.
For purposes of the illustration, total annual costs for a 57-year old woman with breast cancer were
estimated to be $170,229.41.
22,23
The costs of cancer care are highest following diagnosis. The main
sources of costs for the enrollee’s treatment during the first three months were physician services,
imaging, and surgery.
24
The 3-month plan offered by this issuer did not cover outpatient prescription
drugs, though it did offer a discount card. The scenario does not call for the enrollee to incur any
outpatient prescription drug costs within the first three months of treatment.
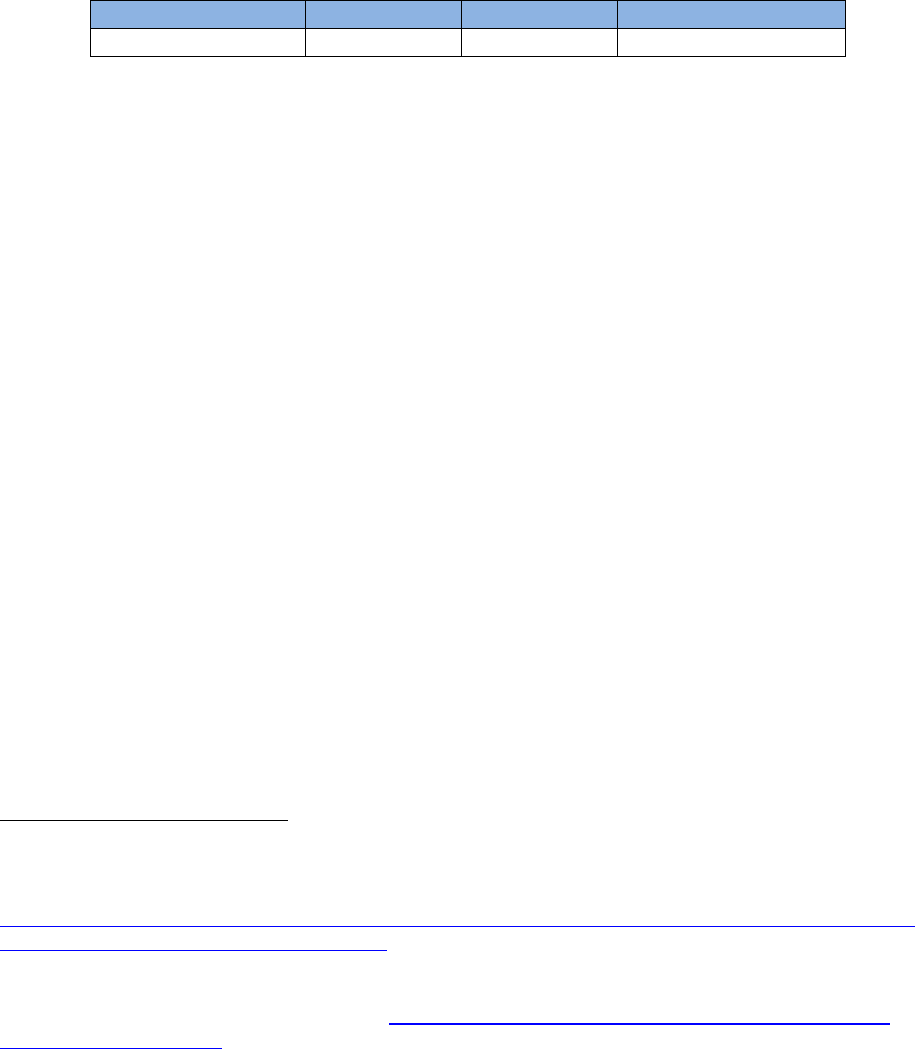
Assuming that the enrollee was able to access all services in-network and further assuming no delays in
treatment, the plan would cover a little less than $60,000 in services during the three months this
individual had coverage. She would then become ineligible for coverage for her cancer care in a
subsequent short-term policy because her cancer diagnosis would be considered a pre-existing
condition. The enrollee’s share of the treatment for the year would amount to over $111,000 –
excluding premiums (which would total $363.90 for the three months of coverage). This would be
20
More information on services contained in the Cost of Cancer report is available in Appendix B.
21
As noted earlier, short-term plan premiums available for this analysis do not reflect medical underwriting,
meaning that actual premiums may be higher.
22
For purposes of this illustration, the “costs” referred to estimated costs for services used for ACS CAN’s Cost of
Cancer report. More information is available at Appendix B.
23
Unless otherwise stated, the term “costs” refers to total annual costs.
24
For purposes of this illustration it is assumed that surgical procedures would include prescription drugs, which
would be covered as part of the bundled payment for the surgical procedure. It is not possible from publicly
available documents to determine whether surgical procedures would be billed as a bundled payment.

13
unaffordable for most Americans.
Nearly half of all American adults
report being unable to cover an
emergency expense costing $400
without having to borrow or sell
something to do so.
25
In the first month of coverage the
plan paid less than $200, leaving the
enrollee to pay more than $8,000,
which was still less than her $12,500
deductible. This 3-month plan
covered only 35 percent of the
enrollee’s costs, mostly due to the
fact that the plan did not provide any
services beyond the first three
months.
After three months the enrollee could not obtain coverage for her cancer treatment from the same
issuer. The issuer’s brochure said it will not cover benefits for a health condition discovered under a
prior plan. Because the end of the three months of short-term coverage is not considered a qualifying
event, the person would unlikely be eligible to enroll in ACA-compliant coverage, likely leaving her
uninsured—while in active cancer treatment—until the next ACA open enrollment period.
As a point of comparison, if the individual enrolled in an ACA plan, her plan would provide coverage for
benefits not covered by the short-term plan (such as prescription drugs). The ACA plan would be
required to cap her in-network cost sharing each year at $7,900.
3-month plan
ACA Plan
Annual Limit
Savings by
choosing an
ACA Plan
Total out-of-pocket costs
(excluding premiums)
$111,128.43 $7,900 $103,228.43
The phrase “ACA plan annual limit” refers to the Affordable Care Act’s annual limit total out-of-pocket expenses an enrollee
would incur for in-network covered services.
25
Board of Governors of the Federal Reserve. (2016, May). Report on the Economic Well-Being of U.S. Households
in 2015. Available at https://www.federalreserve.gov/2015-report-economic-well-being-us-households-
201605.pdf.
$59,100.98
$111,128.43
$363.90
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Plan and Enrollee Cost-Sharing
3-Month Plan
Plan Pays Enrollee OOP costs Enrollee premiums
14
6-Month Plan
We chose to examine a 6-month plan in Florida given that the state has the highest incidence of breast
cancer (among the states examined in this report).
26
The online brokerage site we used gave consumers
several options in which to sort plans. We chose the first 6-month plan that appeared in the
“recommended” sorting option (which is also the default option) offered in Miami-Dade, Florida.
This policy offered coverage for a 57-year old, non-smoking woman as follows:
Monthly Premium
Deductible
Coinsurance
Out
-
of
-
Pocket Limit
$261.76
$10,000
20%
$20,000
This product was an indemnity product, meaning there was no plan network available and that
consumers are responsible for seeking reimbursement directly from the health plan (rather than having
the provider submit claims). More importantly, indemnity plans can expose consumers to additional
costs because the plan will provide limited reimbursement based on a set formula, regardless of the
actual amount billed. In many situations this means the patient’s doctor will bill the patient for the
amount the insurer did not pay (called balance billing).
27
Because we could not quantify the amount of
any balance billed services, for purposes of this illustration we assumed the enrollee would not incur any
additional costs as a result, even though in reality she probably would.
The issuer’s brochure specifically noted that enrollees would not be entitled to receive any benefits for
cancer during the first 30-days of coverage (it was the only issuer examined that had a 30-day waiting
period for cancer-related services). The enrollee incurred over $8,000 in costs in the first month.
The issuer offers consumers the choice of back-to-back policies (e.g., stacked policies), as long as they
are purchased together. According to the brochure, any medical conditions that may arise under the
initial policy would be covered under new certificates, subject to plan limitations (including a higher
premium). For purposes of this illustration we assumed the consumer chose to purchase one 6-month
policy and at the time of purchasing her initial coverage did not purchase a second (stacked) 6-month
policy. As with the example under the 3-month plan, she may not qualify for a special enrollment period
to enroll in ACA coverage until the next open enrollment period, leaving her potentially uninsured until
that time.
26
In 2019, the estimated number of new cases of female breast cancer among the states examined in this report
are as follows: Florida (19,130), Illinois (11,560), Maine (1,390), Pennsylvania (12,070), Texas (18,750) and
Wisconsin (5,270). American Cancer Society. (2019). Cancer Facts & Figures 2019. 5. Available at
https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-
figures/2019/cancer-facts-and-figures-2019.pdf.
27
Short-term plans that do not use a provider network increase the risk of enrollees being faces with significant
balance billing charges. Goe, C. L. (2019, April 30). “Short-term plans: no provider networks lead to large bills for
consumers.” Commonwealth Fund. Available at https://www.commonwealthfund.org/blog/2019/short-term-
plans-large-bills-consumers.

15
For purposes of the illustration, total annual
estimated costs for a 57-year old woman with
breast cancer were $170,229.41. Assuming
that the enrollee was able to access all
services without being subject to balance
billing, the plan would cover roughly
$107,000 of the enrollee’s yearly treatment.
The enrollee would incur more than $63,000
in cost-sharing related to her treatments, and
an additional $1,570.56 in premiums.
While the 6-month plan would cover more of
the enrollee’s expected costs than the 3-
month plan discussed above, it is important
to note that even under this scenario, the
enrollee would still be responsible for cost-sharing (including premiums) of approximately $65,000 – a
cost well out of the reach of most Americans.
As a point of comparison, if the individual enrolled in an ACA plan, her plan would provide coverage for
benefits not covered by the short-term plan (such as prescription drugs). The ACA plan would be
required to cap her in-network cost sharing each year at $7,900.
6-month plan
ACA Plan
Annual Limit
Savings by
choosing an
ACA Plan
Total out-of-pocket costs
(excluding premiums)
$63,019.26 $7,900 $55,119.26
The phrase “ACA plan annual limit” refers to the Affordable Care Act’s annual limit total out-of-pocket expenses an enrollee
would incur for in-network covered services.
12-Month Plan
We chose a 12-month plan offered in Houston, Texas because this plan required the highest premium
($2,598.78 per month) among all 12 areas examined. We wanted to ascertain whether purchasing a plan
with a higher premium provided an enrollee with more robust coverage.
This policy offered coverage for a 57-year old, non-smoking woman as follows:
Monthly Premium
Deductible
Coinsurance
Out
-
of
-
Pocket Limit
$2,598.78
$1,000
50%
$6,000
This plan also had features of an indemnity plan which exposes enrollees to additional cost-sharing for
balance billing which was not quantifiable for purposes of this analysis. This policy stated that enrollees
would incur a $50 copayment for physician services (for both primary care and specialists), though the
$106,709.35
$63,019.26
$1,570.56
0%
20%
40%
60%
80%
100%
Plan and Enrollee Cost-Sharing
6-Month Plan
Plan Pays Enrollee OOP costs Enrollee premiums

16
brochure indicated subsequent visits would be subject to the plan deductible and coinsurance, without
specifically defining a coinsurance related to physician services. Given the relatively low out-of-pocket
limit, under the illustration the enrollee would have only had one physician visit before hitting the cap.
While this policy had a lower out-of-pocket cap
compared to other short-term plans examined, the
brochure noted that the cap did not include the
deductible. Also, while the premiums were significant,
the plan only covered prescription drugs when
prescribed on an inpatient basis for a covered disease
or sickness. The plan did, however, indicate that it
offered an outpatient prescription drug discount
program, though provided no information regarding
the program or its formulary.
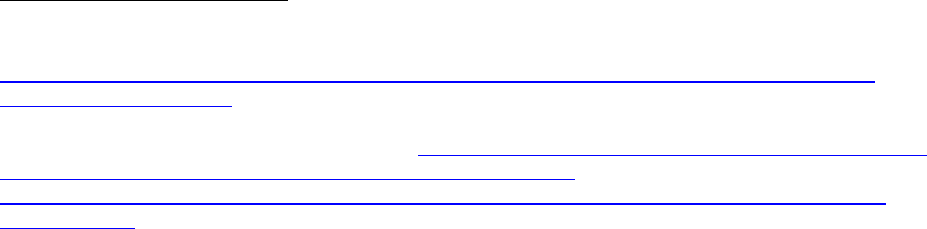
Of the three plans examined, the 12-month plan
provided the most coverage.
28
However, this plan still
left the enrollee with over $40,000 in cost-sharing, not
including monthly premiums which totaled $31,184.52
over the 12-month period. Taken together, the enrollee’s cost-sharing and monthly premiums totaled
$71,886.95, which is actually higher than what the illustrative patient would pay under a 6-month plan
scenario.
As a point of comparison, if the individual enrolled in an ACA plan, her plan would provide coverage for
benefits not covered by the short-term plan (such as prescription drugs). The ACA plan would be
required to cap her in-network cost sharing each year at $7,900.
12-month plan
ACA Plan
Annual Limit
Savings by
choosing an
ACA Plan
Total out-of-pocket costs
(excluding premiums)
$40,702.43 $7,900 $32,802.43
The phrase “ACA plan annual limit” refers to the Affordable Care Act’s annual limit total out-of-pocket expenses an enrollee
would incur for in-network covered services.
28
This statement is predicated on the assumption that the 12-month plan provided robust coverage of physician
services. The authors are unable to verify this claim given the lack of transparency regarding the plan’s coverage of
services.
$129,526.9
8
$40,702.43
$31,184.52
0%
20%
40%
60%
80%
100%
Plan and Enrollee Cost-Sharing
12-Month Plan
Plan Pays Enrollee OOP costs Enrollee premiums

17
Consumer Disclosure Materials
In order to assess coverage options, consumers need information regarding what the policy does and
does not cover, as well as any expected cost-sharing for covered services. Insurance concepts can be
challenging for consumers to understand, and thus any information intended for consumers should be
presented in a clear and concise manner so consumers can assess their coverage options and make an
apples-to-apples comparison. One recent study suggests that consumers are confused by the limitations
of short-term plans because they have been shaped by their experiences and expectations of the
insurance market since the enactment of the ACA and expect all insurance coverage to contain
important patient protections.
29
Lack of Summary of Benefits and Coverage: Under the ACA, plans – including grandfathered plans
30
– are
required to provide enrollees (and potential enrollees) with a Summary of Benefits and Coverage (SBC)
that provides an easy-to understand, standardized summary of the benefits provided under the plan,
including prescription drug formulary information.
31
Short-term plans do not have to comply with this requirement, which makes it harder for consumers to
assess materials that describe what services are, and are not, covered under the plan prior to purchasing
coverage. Indeed, most of the details about plan coverage were said to be included in the plan’s policy
documents, which were not made available to individuals shopping for coverage.
Lack of formulary information: Qualified Health Plans (QHPs) – ACA-compliant plans in the individual
and small group markets – are required to provide consumers with prescription drug coverage as well as
information regarding a plan’s prescription drug formulary (i.e., list of covered drugs). Three of the
issuers examined in this report did not provide any coverage of outpatient prescription drugs. One issuer
noted under its excluded benefits page that outpatient prescription drugs were not covered unless
shown as included in the Schedule of Benefits, which was not available to consumers shopping for
coverage.
Another issuer provided prescription drug coverage for some plan options but not for others. While the
brochure supplied by the issuer noted that outpatient prescription drugs would be subject to a separate
prescription drug deductible, it did not provide access to any formulary information. However, the
brochure noted that no specialty drugs were covered under any plan offered by the issuer. Many cancer
drugs are considered specialty drugs.
32
29
Consumer Representatives to the National Association of Insurance Commissioners. (2019, Mar. 15). New
Consumer Testing Shows Limited Consumer Understanding of Short-Term Plans and Need for Continued State and
NAIC Action. Available https://healthyfuturega.org/wp-content/uploads/2019/04/Consumer-Testing-Report_NAIC-
Consumer-Reps.pdf.
30
A “grandfathered health plan” is a policy that was purchased before March 23, 2010. These plans are exempt
from many of the protections provided under the Affordable Care Act.
31
45 C.F.R. § 147.200.
32
Most cancer drugs (such as chemotherapy) are considered specialty drugs because they often require special
handling, administration, and/or monitoring. Depending on the insurer and the type of chemotherapy, these drugs
can be covered under a plan’s medical benefit, not the plan’s prescription drug benefit.

18
Finally, another provided confusing information regarding prescription drug coverage. The brochure
seemed to indicate that one out of the four plan options does not cover prescription drugs – offering
only a discount card. The remaining three plan options seemed to indicate the plan provided some drug
coverage, though the brochure did not mention any formulary information. Consumers were told to pay
for their prescriptions at the point of sale “at the lowest price available” and to then submit a claim to
the plan for reimbursement. Even then, the brochure indicated that the issuer imposed a maximum
$3,000 benefit for prescription drugs. However, in the exclusions section of the brochure, the issuer
explicitly stated, “no benefits are payable for expenses … for outpatient prescription drugs, except as
provided for in the policy/certificate.” Neither the policy nor the certificate was made available to
individuals shopping for coverage.
Disclaimer: All of the examined issuer brochures included a disclaimer of some kind. These disclaimers
all noted that the coverage provided does not qualify as minimum essential coverage as required under
the Affordable Care Act. Four issuers’ disclaimers noted that not having minimum essential coverage
could result in a federal tax penalty.
One issuer included a disclaimer noting that short-term plan coverage does not constitute minimum
essential coverage, followed by a statement that the plan “can, however, offer financial protection in
the event of an unexpected injury or illness when you are waiting for coverage to begin under an ACA-
compliant plan.” Most cancer diagnoses are unexpected. The disclaimer offered by this issuer implies
that the policy would provide coverage for an unexpected illness, yet as our analysis demonstrated, the
coverage proved inadequate with respect to a diagnosis of breast cancer. The 12-month plan discussed
in detail above, offered by this issuer would leave a patient with over $40,000 in out-of-pocket costs
(excluding premiums).
Preventive Services
Cancers that are found at an early stage through screening are less expensive to treat and lead to
greater survival.
33
Providing access to high quality primary medical care and preventive services is one of
the most effective ways to prevent or detect cancer at an earlier, more curable, and less expensive
stage. ACA-compliant plans are required to cover without cost-sharing clinical preventive services that
receive an “A” or a “B” rating from the United States Preventive Services Task Force (USPSTF) as well as
vaccines recommended by the Advisory Committee on Immunization Practices (ACIP). These services
include breast, cervical colorectal, and lung cancer screenings, tobacco cessation treatment, weight loss
interventions to reduce obesity, and a vaccine that prevents cervical and other cancers.
Cancer screenings: It was very hard to ascertain whether the issuers covered routine cancer screenings
of any kind. Only two issuers noted in their plan brochures that they offered coverage for any cancer
screenings. Neither of these issuers offered coverage for all the cancer screenings recommended by the
USPSTF. Of the two issuers who provided any cancer screening coverage, one issuer’s brochure notes
33
American Cancer Society. (2017). Cancer Prevention & Early Detection Facts & Figures 2016-2017.

19
that it covers mammography, pap smear, and prostate antigen test, though did not provide additional
information regarding the intervals at which these services would be covered
34
and whether any cost-
sharing would be imposed. The other issuer’s brochure noted that it covered colorectal cancer screening
examinations, prostate specific antigen testing, and any preventive services required by the state.
35
Tobacco cessation products: Quitting tobacco use can often require multiple quit attempts and
treatment is more likely to be successful with the use of scientifically-effective treatments including
prescription medications. Four of the six issuer brochures explicitly note they do not provide coverage
for tobacco cessation products. While the remaining two issuer brochures did not specifically mention
coverage for tobacco cessation products, neither of these issuers provide coverage for out-patient
prescription drugs.
Wellness exams: Short-term plans are not required to cover physical exams. In reviewing plan
brochures, only one issuer explicitly noted that “wellness exams” were covered for a $50 copayment.
However, with respect to the other issuers there were inconsistencies between the information
provided in the plan brochures and the information available in the “details” page displayed by the
online broker. For example, another issuer’s brochure exclusions and limitations section expressly states
that it does not cover costs for routine physical exams or other services not needed for medical
treatment, but the “details” page provided by the online broker states that preventive health exams are
covered on a limited basis.
34
The USPSTF screening recommendations provide specific screening intervals. For example, the USPSTF
recommends screening for cervical cancer in women age 21 to 65 every three years. U.S. Preventive Services Task
Force. Cervical Cancer: Screening. Release date Aug. 2018.
35
This issuer used a multi-state brochure which made it confusing for consumers to gain a better understanding of
what is covered under a specific plan option.

20
ACS CAN Recommendations
Proponents of short-term plans often claim these products are not intended for all consumers but
rather offer a more affordable option than the robust ACA marketplace plans. While premiums for
short-term plans are generally lower relative to ACA plans, our analysis shows that short-term plans
actually expose enrollees with serious illnesses to higher out-of-pocket cost. These costs can be tens of
thousands of dollars which is far beyond the financial means of most Americans.
Research suggests that consumers generally do not understand short-term plans’ limitation on covered
benefits,
36
particularly given that they have become accustomed to, and now expect the patient
protections provided under the ACA (such as the prohibition of medical underwriting). Some of this
confusion may be due to how these plans are marketed. As noted earlier, one issuer’s disclaimer
specifically noted that the product was intended to offer financial protection for an unexpected illness.
Yet our analysis showed the short-term plans included in this report exposed the enrollee to significant
out-of-pocket costs associated with an unexpected diagnosis of breast cancer.
We also note that the short-term plans examined in this report failed to provide information necessary
to determine an enrollee’s out-of-pocket costs and coverage of benefits related to an individual’s cancer
treatment. For example, we were not able to ascertain the exact premiums an individual would pay if
she enrolled in a short-term plan because the premiums made available to those shopping for coverage
did not reflect medical underwriting.
Short-term plans are allowed to deny coverage based on an individual’s pre-existing conditions – in
many cases whether or not those pre-existing conditions were known at the time coverage was sought.
This allows short-term plans to discriminate against individuals with high health care costs.
Even if an individual were able to pass medical underwriting and obtain coverage under a short-term
plan, the plans examined in this report failed to provide sufficient coverage for the products and services
cancer patients need for their treatment. Indeed, many of the short-term plans failed to provide
comprehensive access to preventive services, which are key to diagnosing cancer at an earlier stage
when an individual has a greater likelihood of a successful outcome. Half of the short-term plans
examined in this report did not provide any coverage of outpatient prescription drugs. Of the plans that
indicated there was some prescription drug coverage, none of the plans provided information on the
plan’s formulary. The issuers’ brochures would often refer to a Schedule of Benefits or other policy
documents, which were not provided to individuals shopping for coverage.
Short-term plans also have a negative impact on the risk pool for ACA-compliant plans. Short-term plans
tend to attract younger, healthier individuals who are lured by the plans’ lower premiums and more
likely to be approved for coverage given their health status. As a result, older and sicker individuals are
left in the ACA-compliant plan risk pool, which results in increased premiums for those plans. As
36
Consumer Representatives to the National Association of Insurance Commissioners. New Consumer Testing
Shows Limited Consumer Understanding of Short-Term Plans and Need for Continued State and NAIC Action.
21
premiums become more expensive, individuals, particularly those who do not qualify for subsidies, are
more likely to forego coverage due to cost.
Policymakers should consider prohibiting the sale, or at the very least limiting the availability of short-
term plans because of the inadequacy of their coverage, combined with the negative impact on the risk
pool and availability of coverage in the ACA-compliant market. Since the Administration’s final rule
which expanded access to short-term plans went into effect, there has been a significant increase in the
length of coverage for short-term plan options, which can be confusing to consumers who may mistake
these plans for comprehensive, ACA-compliant coverage.
While the federal government finalized a rule expanding access to these plans, there are a number of
states that have taken action to address the concerns raised by the proliferation of short-term plans.
37
Some states have enacted policies that prohibit short-term plans from engaging in medical underwriting,
and other states have enacted limits on the length of time a consumer could be enrolled in a short-term
plan.
38
Action taken by states to strengthen their markets should be encouraged but ultimately result in
a patchwork of consumer protections. Strong federal protections limiting the duration and availability of
short-term plans are needed to ensure that all consumers are protected.
37
Palanker D, Kona M, Curran E. (2019, May 2). “States step up to protect insurance markets and consumers from
short term health plans.” Commonwealth Fund. Available at
https://www.commonwealthfund.org/publications/issue-briefs/2019/may/states-step-up-protect-markets-
consumers-short-term-plans.
38
Giovannelli J, Lucia K, Corlette S. (2019, Feb). “What is Your State Doing to Affect Access to Adequate Health
Insurance?” The Commonwealth Fund. Available at https://www.commonwealthfund.org/publications/maps-and-
interactives/2019/mar/what-your-state-doing-affect-access-adequate-
health?redirect_source=/publications/maps-and-interactives/2019/feb/what-your-state-doing-affect-access-
adequate-health.
22
Acknowledgements
This work was authored by Anna Schwamlein Howard, Policy Principal, American Cancer Society Cancer
Action Network.
The author gratefully acknowledges the input of Keysha Brooks-Coley, Alissa Crispino, Stephanie
Krenrich, Lisa A. Lacasse, Allison Miller, Cathy Peters, Jennifer Singleterry, Kirsten Sloan, Carter Steger,
Pam Traxel and David Woodmansee at the American Cancer Society Cancer Action Network and Robin
Yabroff at the American Cancer Society.
The author also would like to thank Jean Hearne, Katie Keith, Sarah Lueck, Karen Pollitz for their valuable
insights.

23
Appendix A
For purposes of this report, the author visited a well-known online brokerage website and searched for
short-term, limited-duration health plans using the patient profile of a 57-year-old woman, who
indicated she was a non-smoker. Plan information was sought using the following zip codes:
City State
Zip Code
Urban/Rural
Chicago IL
60639
Urban
LaSalle IL
61301
Rural
Houston TX
77051
Urban
Mission TX
78572
Rural
Portland ME
04103
Urban
Allagash ME
04774
Rural
Miami-Dade FL
33172
Urban
Jackson FL
32446
Rural
Milwaukee WI
53202
Urban
Waupaca WI
54981
Rural
Pittsburgh PA
15286
Urban
Towanda PA
18848
Rural
Plan information was solicited in November 2018 for five states. Plan information for Pennsylvania was
solicited in March 2019.
Information regarding premiums, deductibles, and plan duration was based on the index provided by
the online broker. In addition, the authors selected specific plans – including the least expensive and
most expensive plans in each of the zip codes examined. The author recorded the online broker’s
summary information regarding the plan. The broker’s summary information also contained direct links
to the issuer’s plan brochure and plan exclusions and exceptions. For all but one issuer included its
plan’s exclusions within the plan brochure. This issuer provided plan exclusion information as a separate
document, accessible via a separate link.

24
Appendix B
In September-December 2016, experts at Avalere Health, LLC, the American Cancer Society and the
American Cancer Society Cancer Action Network (ACS CAN) created three profiles of cancer patients
and treatment regimens. Avalere analysts ran each patient profile through three insurance scenarios
and calculated patient out-of-pocket costs and total healthcare costs. These profiles can be found at
https://www.fightcancer.org/policy-resources/costs-cancer. Following is detailed methodology for
the breast cancer patient profile, Mary.
Mary had Stage I breast cancer. She had one tumor that measured 1 cm in size. Her breast cancer was
hormone-receptive positive and HER2 negative. Her RT-PCR score was 20, which meant that her
cancer might come back, so Mary chose to have adjuvant chemotherapy. Her oncologist also
recommended radiation treatment to stop her cancer from returning. Mary was assumed to be
diagnosed in the first month of coverage of each of the plans examined in this report. Mary’s
treatment regimen was based on National Comprehensive Cancer Network (NCCN) Guidelines for
patients with Mary’s profile. The treatment regimen included:
• Mammogram
• Ultrasound
• CBC and liver function tests
• Breast MRI
• Core needle biopsy
• Lumpectomy (surgery)
• Sentinel lymph node biopsy
• Hormone receptor and oncotype tests
• Chemotherapy – dose-dense AC and paclitaxel
• Supportive care drugs – filgrastim, aprepitant, dexamethasone, ondansetron
• Monitoring blood tests
• EBRT (radiation)
• Adjuvant hormone therapy – letrozole
• Multiple primary care provider visits
• Multiple specialist visits with a medical oncologist, radiation oncologist, breast surgeon
Individual Market Insurance Scenario
The treatment costs used in this model were average commercial costs across private payers taken
from MEPS and HCUP data sets. 2014 was the most recent year available for these data sets at the
time of the analysis of the Cost of Cancer report. In instances where commercial rates were not
available, 100 percent of published 2016 Medicare rates from the following fee schedules were used:
Medicare Physician Fee Schedule, Outpatient Prospective Payment System, Inpatient Prospective
Payment Systems, and Clinical Lab Fee Schedule.

25
The costs used in this model for pharmacological treatments are as follows. For intravenous drugs,
average sales price (ASP) data from the Centers for Medicare and Medicaid Services (CMS) October
2016 pricing file were used, reflecting ASP plus 6 percent. Though some plans may reimburse based
on other methodologies, their methodologies are not always made publicly available, which creates
challenges in estimating precise payment amounts; using the Medicare rate should serve as a
reasonable estimate for most payers. For oral drugs, prices were obtained from the Medicare Plan
Finder, assuming the patient lived in Texas zip code 77025. These data were used to represent
negotiated prices similar to those negotiated by an insurance plan.
It was assumed that all treatment received was in-network and covered – note that patient costs
would likely increase with out-of-network or non-covered treatments.
The Costs of Cancer: Addressing Patient Costs report and accompanying materials can be found at
https://www.fightcancer.org/policy-resources/costs-cancer.
