
Public Health Pest Control
APPLICATOR TRAINING MANUAL
Florida Department of Agriculture and Consumer Services
3125 Conner Boulevard
Tallahassee, Florida 32399-1650

Public Health Pest Control
APPLICATOR TRAINING MANUAL
Florida Department of Agriculture and
Consumer Services
3125 Conner Boulevard
Tallahassee, Florida 32399-1650

Acknowledgements
In accordance with Florida Administrative Code
Chapter 5E-13.040, all persons who apply or supervise
the application of a pesticide intended to control
arthropods on property other than their own individual
residential or agricultural property must be licensed to
do so with a Public Health Pest Control (PHPC) license
or work under the supervision of a licensed applicator.
In order to obtain the PHPC license, applicants must
score 70% or above on two exams administered by the
Florida Department of Agriculture and Consumer
Services (FDACS): the General Standards (Core) exam
and the Public Health Pest Control exam. This Public
Health Pest Control Manual, in conjunction with the
Core Manual “Applying Pesticides Correctly” published
by University of Florida, will provide general
information necessary to meet U. S. Environmental
Protection Agency and Florida standards for
certification as a pesticide applicator in the commercial
category, Public Health Pest Control.
The original Public Health Pest Control Manual
was prepared by Elisabeth Beck of the Florida
Department of Health and Rehabilitative Services
(HRS), Office of Entomology. Technical assistance was
provided by Dr. Andrew Rogers, retired, HRS, and the
late Dr. Maurice Provost, Florida Medical Entomology
Laboratory. The manual was edited and produced by
the IFAS Editorial Department under the supervision of
JoAnn Pierce. Appreciation is expressed to the U. S.
Department of Health and Human Services (USHHS),
and to extension specialists in neighboring states for
valuable ideas and visual aids. Credit is due to the late
Paul J. Hunt, and John Gamble, East Volusia Mosquito
Control District, and Thomas M. Loyless, Bureau of
Entomology and Pest Control (BEPC) of FDACS for
photographs of equipment and habitats.
Thanks are due to Dr. Carlyle B. Rathburn,
retired, John A. Mulrennan, Sr. Public Health
Entomology Research and Education Center for the
section on calibration of equipment, Dr. Philip Koehler,
Department of Entomology and Nematology, IFAS,
University of Florida, and William R. Opp, retired, Lee
County Mosquito Control District for additional
technical assistance.
The last edition was updated and revised in May
2001 by Thomas M. Loyless, FDACS, with assistance
from Edsel M. Fussell, Florida Keys Mosquito Control
District, Mark Latham, Manatee County Mosquito
Control District and Stephen Sickerman, FDACS
(currently with the South Walton Mosquito Control
District).
This edition was updated and revised in 2011 by
Dr. Yongxing “Peter” Jiang, with assistance from Dr.
Dave Daiker, Angela Weeks-Samanie, and Joe Claborn of
the Florida Department of Agriculture and Consumer
Services, Dr. Jeff Stivers, Collier Mosquito Control
District, and Dr. Rui-de Xue, Anastasia Mosquito Control
District.
The Department would like to extend a special thanks to Joe Claborn for the
cover photograph of the St. Marks River and mosquito breeding habitats.
i

Table of Contents
Acknowledgements .................................................................................................................................................. i
Introduction .............................................................................................................................................................. 1
History of Mosquito Control in Florida ............................................................................................................... 1
Anti-Mosquito Association ..................................................................................................................................... 1
Formed ............................................................................................................................................................. 1
Division of Entomology Created ................................................................................................................ 2
Entomological Research Center Established .......................................................................................... 2
Mosquitoes ................................................................................................................................................................ 3
How to Recognize a Mosquito .................................................................................................................... 3
Classification .................................................................................................................................................. 3
Importance to Health and Economy ......................................................................................................... 3
Mosquito Species in Florida ................................................................................................................................... 4
Mosquitoes and Their Production Sites in Florida ..................................................................................... 5-12
Identification ........................................................................................................................................................... 12
Larval Morphology ...................................................................................................................................... 15
Adult Morphology ....................................................................................................................................... 15
Some Problem Species of Mosquitoes in Florida ............................................................................................ 16
Common Problem Mosquitoes ................................................................................................................. 16
Other Problem Mosquitoes ....................................................................................................................... 16
Mosquito Control Practice ................................................................................................................................... 20
Responsibilities of a Mosquito Control Director .................................................................................. 20
Continuing education ................................................................................................................................. 20
Planning the Project.................................................................................................................................... 21
Equipment for Mosquito Control ............................................................................................................. 23
Larviciding Equipment ............................................................................................................................... 23
Adulticiding Equipment ............................................................................................................................. 23
Calibration of ULV Machines and Checking Droplet Size ................................................................... 23
Calibration of Thermal Fog Equipment .................................................................................................. 24
Maintenance of Equipment ....................................................................................................................... 24
Methods of Mosquito Control .............................................................................................................................. 24
Premise Sanitation ...................................................................................................................................... 24
Land and Water Management .................................................................................................................. 24
Chemical Control ......................................................................................................................................... 25
Larvicides ........................................................................................................................................... 25
Adulticides.......................................................................................................................................... 25
Other Control Methods .............................................................................................................................. 26
Legal Aspects of Mosquito Control..................................................................................................................... 27
Public Relations and Managing Negative Impacts.......................................................................................... 27
Arthropods of Public Health Importance ......................................................................................................... 28
Control of Other Arthropods by Mosquito Control Districts ....................................................................... 29
Sand Flies ............................................................................................................................................ 30
Stable Flies ......................................................................................................................................... 30
Blind Mosquitoes .............................................................................................................................. 30
House Flies ......................................................................................................................................... 30
Eye Gnats ............................................................................................................................................ 30
Miscellaneous Insects ...................................................................................................................... 30
Glossary .................................................................................................................................................................... 32
Bibliography ............................................................................................................................................................ 34

Figure 1. Florida and its counties

Introduction
The State of Florida has made great progress
in reducing the hordes of malaria-carrying Anopheles
and salt marsh mosquitoes which, in years past,
harassed visitors and Floridians alike. Many miles of
salt marsh stretching down the east and west coasts of
the State have been ditched or impounded by the
mosquito control districts, making the coastal areas
habitable and opening them to development for housing
and as tourist resorts.
There is no question that the control of salt
marsh mosquitoes has made a major contribution to the
development of the tourist industry in this state;
without this control, tourists would not have repeatedly
visited to enjoy the beaches and attractions. Figure 2
gives a good picture of the relationship, showing the
steady rise in income from tourism plotted against the
steady decline of the major salt marsh pest mosquito,
Aedes taeniorhynchus.
Mosquitoes occur throughout the world,
breeding in almost every known aquatic habitat except
very swift currents and in open bodies of water.
Wherever they occur, mosquitoes are, for humans, at
best an annoyance and at worst vectors of deadly
diseases. Over 3,000 species have been described
worldwide and they display a broad range of habitats.
Larvae may be found in such diverse places as the
grassy margins of ponds, land crab holes, and aquatic
plants. Depending on the species, eggs may be laid
singly or in rafts, on water or on damp soil where they
hatch in subsequent flooding. Flight ranges also vary
among species from a few hundred feet to more than
eighty miles with favorable winds. Hibernation or
overwintering in different species may be in the egg
stage, as larvae, or as adults. Each of these variations
among species can affect the efficiency of any measure
utilized to control them.
Figure 2. Average number of female Aedes
taeniorhynchus per light trap
History of Mosquito Control in Florida
Florida is the leading tourism destination in
the United States, and, in terms of dollars spent, it is the
number one vacation destination in the world.
Florida, with more than 1,200 miles of
coastline, a warm subtropical climate, and heavy
rainfall, produces an unusually rich fauna, including 80
species of mosquitoes.
We often forget that Florida was not always a
vacation paradise where people could escape for
warmth, recreation and relaxation. As little as 100 years
ago, many parts of Florida were considered unbearable,
thanks in large part to legions of mosquitoes. Pestilence
and disease raged, and many people said the State could
not be developed. When Congress was debating the
merits of statehood for Florida, John Randolph of
Virginia stated that Florida could never be developed,
nor would it ever be a fit place to live. He described the
1
land as a "land of swamps, of quagmires, of frogs and
alligators and mosquitoes."
The battle with the mosquito, however, was a
long, tough fight and there were many casualties. The
mosquito was such a plague when the Spaniards arrived
that they named what today is Ponce de Leon Inlet,
"Barro de Mosquitoes." Since the time of the earliest
maps, some of Florida's inlets, lagoons, and sections
have borne the name Mosquito. In the 18th Century, the
part of Florida lying between the St. Johns River and the
coastal lagoons north of Cape Canaveral was called "The
Mosquito Country," or "The Mosquitoes."
In 1824, when Mosquito Country became a
county which included a large portion of peninsular
Florida, government officials could think of no more
appropriate name than "Mosquito County." Today, that
county is known as Orange County and is home for

many of our major attractions in and around Orlando.
For many years settlements in Florida were
restricted to the northern tier of the state. The
peninsular portion of Florida was a series of swamps,
lakes, rivers, and hammocks populated mostly by
hoards of mosquitoes and other biting insects.
Although northern Florida was settled, it was
anything but a pleasant place to live. It suffered from
disease, hardship, and poverty; the major cities of
Jacksonville, St. Augustine, Tallahassee and Pensacola
were known as the "malaria belt."
Summer routinely brought swarms of
mosquitoes and deadly fevers to the region. Commerce
was seriously curtailed and those who could afford it
fled to the north for relief. Those forced to stay behind
faced the threat and certainty of disease. One of the
worst sieges of disease was the yellow fever epidemic in
1877 in Jacksonville and Fernandina Beach. It was
described by historians as the State's worst holocaust.
Fernandina Beach, with a population of 1,632, had
1,146 persons ill with the fever. Twenty-four died. In
1887, yellow fever epidemics raged in Key West,
Tampa, Plant City, and Manatee. The 1888 epidemic in
Jacksonville saw 10,000 persons (out of a population of
26,700 in Duval County) flee the city in carriages, drays,
wagon trains, and ships.
All of that has changed thanks to mosquito
control. Consider, for example, the success story of
mosquito control at Sanibel Island. On Florida's rapidly
expanding southwest coast, Sanibel is one of the resort
jewels our State offers, fantastic weather, incredible
sunsets, great beaches, and fine resorts. Sanibel has it
all. But without mosquito control, it would be virtually
uninhabitable. In fact, the island was once so heavily
infested with mosquitoes that bred in the vast grassy
marshes that the local postman had to make his rounds
in July dressed like an Eskimo in a parka and netting.
Anti-Mosquito Association Formed
No organized effort was made to control
mosquitoes in Florida as a way of preventing malaria
until World War I when the U.S. Army, U. S. Public
Health Service, and the State Board of Health set up a
program of drainage and larviciding at Camp Johnson,
near Jacksonville. In 1919, the State Board of Health, the
city of Perry, and the Burton Swartz Cypress Company
jointly set up a malaria control project in the city of
Perry, one of the most malarious areas of the State. At
that time the Perry project was one of the largest
malaria control projects in the country and was the first
non-military control project in Florida.
Mosquito control in Florida was given impetus
in 1922 by the formation of the Florida Anti-Mosquito
Association (FAMA) (now known as the Florida
Mosquito Control Association, FMCA), with Dr. J. Y.
Porter, the State's first Health Officer, serving as its
president. The Indian River County Mosquito Control
District was established in 1925, followed by St. Lucie
Mosquito District in 1926, Broward County Mosquito
Control District in 1934 and Dade County Mosquito
2
Control District in 1935. By 1975, there were 52
mosquito control districts in Florida, and that number
has remained fairly constant to the present day.
From the depression year of 1933 until funds
were withdrawn in 1941, many malaria control projects
were performed with funding from the Civil Works
Administration, Emergency Relief Administration of the
Works Progress Administration. During this period,
more than 1,500 miles of drainage ditches were dug
throughout the state to eliminate mosquito breeding
habitats.
In 1941, a Bureau of Malaria Control was
created within the Division of Health and in 1942, the
U.S. Public Health Service set up the first Malaria
Control in War Areas project in Florida near
Tallahassee. Similar projects were then established
around all military bases in the state. A program of DDT
residual house spraying in malarious areas of Florida
was supported by U.S. Public Health Funds from 1945
through 1949.
Division of Entomology Created
In 1946, the Bureau of Malaria Control was
abolished and a Division of Entomology was created
within the Bureau of Sanitary Engineering. In 1953, the
Division was raised to Bureau status. In 1976, the
Bureau of Entomology became the Office of Entomology
and in 1986, became Entomology Services in the
Department of Health and Rehabilitative Services. The
program was moved to the Department of Agriculture
and Consumer Services (DACS) in 1992, where it is now
known as the Bureau of Scientific Evaluation and
Technical Assistance (BSETA). The functions of the
BSETA include promoting control of insects of public
health importance, serving as advisors and consultants
for mosquito control districts, and administering all
state funds appropriated for nonagricultural arthropod
control work. State laws were passed in 1925, 1929,
and 1941 which set up methods for establishing self-
taxing mosquito control districts and in 1949, a State
law was passed that provided State aid to districts in
the form of insecticides, materials, equipment,
personnel, and vehicles.
In 1953, the State Legislature passed a second
State aid law whereby any board of county
commissioners or mosquito control district that places
funds in its budget for control of "arthropods of public
health importance", would, upon proper certification,
receive funds directly from the State of up to 75 percent
of the funds appropriated by the county or district.
These funds were to be used for permanent control
measures; additional appropriations were given as
matching funds for either permanent or temporary
control measures.
This act has been amended several times. At
present, it provides that a county or district shall be
eligible, upon approval of the Department of Agriculture
and Consumer Services, to receive state funds. The
amount and type of State aid currently available to
mosquito control agencies is described in Chapter 5E-

13. 030 Florida Administrative Code (F.A.C.)
Entomological Research Center Established
In 1953, the legislature appropriated money to
establish the Entomological Research Center at Vero
Beach to study the biology and control of arthropods of
public health importance in Florida. The center was
dedicated in 1956 and has become world renowned for
the excellence of its facilities and its research. In 1973,
the name was changed to the Florida Medical
Entomology Laboratory and, in 1979, it was transferred
to the University of Florida, Institute of Food and
Agricultural Sciences.
The John A. Mulrennan, Sr. Public Health
Entomology Research and Education Center (JAMS
PHEREC), formally the West Florida Arthropod
Research Laboratory, was established at Panama City in
1963. Its primarily mission was to study the biology and
control of the "dog fly," known elsewhere as the stable
fly (Stomoxys calcitrans), which plagues people on the
Gulf beaches in summer, and to test the efficacy of
various insecticides on mosquitoes and other
arthropods. In 1992, JAMS PHEREC was transferred to
Florida Agricultural and Mechanical University, College
of Engineering Sciences, Technology and Agriculture,
but its overall mission remains unchanged.
MOSQUITOES
How to Recognize a Mosquito
Mosquitoes are insects with long slender
bodies, narrow wings with a fringe of scales on the hind
margin and along the veins, and long, very thin legs. In
females, the elongate proboscis is firm and usually
adapted for piercing and sucking blood. Male
mosquitoes cannot suck blood, and survive on nectar.
Females are also required to feed on nectar of various
plants to obtain sugar for energy, but rely on a blood
meal for egg-laying.
There are four life stages: egg, larva, pupa, and
winged adult. Eggs may be laid singly or in rafts,
deposited in water, on the sides of containers where
water will soon cover them, or on damp soil where they
must undergo a maturing process before they can hatch
when flooded by rainfall or high tides. Mosquitoes of the
genus Mansonia deposit their eggs on the underside,
and, less so, on the upper side of floating aquatic plants
such as water lettuce and water hyacinth. After the eggs
hatch, the larvae or wrigglers begin to feed on very
small plant and animal particles, going through four
growth stages or instars before becoming pupae. With
the exception of species in the genera Mansonia and
Coquillettidia, larvae of other species all breathe air at
the surface of the water. Species of Mansonia and
Coquillettidia, in contrast, have a sharp pointed siphon
which pierces the roots and stems of aquatic plants to
obtain oxygen from the plant. The pupal or tumbler
stage is comparatively brief, does not feed, and is active
only if disturbed. Upon maturation, the pupa emerges
from the surface of the water, splits the chitinous pupal
skin and the adult emerges. After a brief time on the
surface to dry its wings, the adult flies away.
Classification
In order to make it clear exactly which animal
among the many kinds one is speaking or writing about,
scientists have devised a system of classification and
naming in which each kind of animal known to science
is given a name consisting of two words. The first name
is the name of the genus and is written with a capital
3
letter. Mosquito publications, however, often abbreviate
the genus name using a two-letter abbreviation, for
instance, Ae. for Aedes and Cx. for Culex. The second
name is a specific name and begins with a small letter.
Together they form the species name which is always
either italicized or underlined (to indicate italics). The
classification of the mosquito which transmitted
malaria in the southeastern United States is shown
below:
Kingdom - Animalia (all animals)
Phylum - Arthropods (all animals with paired,
jointed appendages and
exoskeletons)
Class - Insecta (all insects; three main body
divisions and six legs)
Order - Diptera (true flies, all two-winged flies
with the hind wings reduced
to knobbed structures called
halteres)
Family - Culicidae (all mosquitoes)
Genus - Anopheles
Species - Anopheles quadrimaculatus Say (Say is the
person who first described the species)
Currently, 80 species of mosquitoes, belonging
to 12 different genera, have been recorded in Florida.
These mosquitoes inhabit a wide variety of aquatic
habitats, and the biology of each of these species is
unique in some way. Unique distinctions between
species include larval habitat, host preferences, and
flight ranges, and will be discussed in more detail in the
section focusing on various mosquito species. The
differences in appearance (morphological differences)
are discussed in the section on identification.
Importance to Health and Economy
In years past, malaria, yellow fever, and
dengue were present in the State in epidemic
proportions. Through mosquito control, these diseases
are now no longer endemic. However, Anopheles

quadrimaculatus, which transmits malaria and Aedes
aegypti, which vectors both yellow fever and dengue,
are still present in large numbers, and if persons
carrying the disease in their bloodstreams should come
into Florida from other areas, it would be possible for
mosquitoes to bite them and become infected. In this
way, a new cycle of these diseases could begin.
Although secondary infections may result
from scratching mosquito bites, and there are people
who are allergic to the bites, the chief medical concern
in Florida at the present time is the possibility of an
arthropod- borne encephalitis epidemic. Viruses of
Eastern Equine Encephalitis, Western Equine
Encephalitis, St. Louis Encephalitis, California
Encephalitis and Venezuelan Equine Encephalitis have
been found in mosquitoes in the State.
Eastern Equine Encephalitis Eastern
Equine Encephalitis (EEE) is an enzootic disease that
was first recognized in Massachusetts, in 1831 when 75
horses died of an encephalitic illness. The casual agent,
Eastern Equine Encephalitis virus (EEEV), is an
alphavirus that was first isolated from infected horse
brains in the 1930s and currently occurs in focal
locations of the eastern United States including Florida.
EEE is capable of infecting a wide range of animals
including mammals, birds, reptiles and amphibians. The
virus is maintained in natural cycles involving birds and
Culiseta melanura in freshwater swampy areas with a
peak of activity between May and August. In this usual
cycle of transmission, the virus does not escape from
the swampy areas because the mosquito species,
Culiseta melanura, prefers to feed upon birds and does
not usually bite humans or other animals. However,
transmission of EEEV to mammals occurs via bridge
vectors because they bring the virus from avian
populations to mammalian populations. These bridge
vectors include Coquillettidia perturbans, Aedes
atlanticus, Culex nigripalpus, Cx. quinquefasciatus and
Aedes solicitants. These species feed on both birds and
mammals and can transmit the virus and cause disease
in people, horses, dogs and some birds such as
pheasants, quail, ostriches and emus.
Most persons infected with EEEV have no
apparent illness. However, symptoms of severe cases of
EEE include sudden onset of headache, high fever, chills,
and vomiting. The illness may then progress to
disorientation, seizures, or coma. EEE is one of the most
severe mosquito-transmitted diseases in the United
States with approximately 33% mortality and
significant brain damage in most survivors.
Despite there having been only 81 human
cases documented in Florida in the past fifty years
(1957-2008), the State averages over 70 reported
equine cases each year. In years when conditions favor
the spread of EEE, the number of reported cases can
exceed 200, with over 90% of the affected horses dying.
The distribution of EEE cases have predominantly been
in areas north of Lake Okeechobee, including panhandle
areas (Walton, Holmes, Jackson, Leon, Jefferson,
Madison and Escambia Counties); the lower St. Johns
River areas (Duval, Volusia, Flagler, Putnam and Clay
Counties); and the green swamp region area (Lake,
Orange, Pasco, Polk, Osceola, Pinellas, Hillsborough and
Manatee Counties).
A vaccine is available for horses, but not for
humans. Preventive measures should include effective
mosquito control and avoidance of mosquito bites by
using insect repellent, wearing protective clothing, and
staying indoors while mosquitoes are most active.
St. Louis Encephalitis St. Louis
Encephalitis (SLE) was first recognized in the vicinity of
St. Louis, Missouri and the neighboring St. Louis County
in 1933 when an encephalitis epidemic broke out. Over
1,000 cases were reported to the local health
departments and the newly constituted National
Institute of Health. St. Louis encephalitis virus (SLEV), a
flavivirus, is one mosquito-transmitted viral disease
that is of great medical importance in North America.
During summer, SLEV is maintained in a mosquito-bird
cycle, with periodic amplification by birds and Culex
mosquitoes.
Normally less than 1% of SLEV infections in
humans are clinically apparent and the vast majority of
infections remain undiagnosed. The occurrence and
severity of SLE in humans is strongly dependent on age.
The case fatality rate in Florida SLE epidemics has
ranged from 4-30 percent. Deaths were almost
exclusively among people age 50 and older. It is not
uncommon for those surviving severe cases of SLE to
suffer long-term residual neurological damage, which
include paralysis, memory loss, or deterioration of fine
motor skills.
Major SLE outbreaks occurred in Florida in
1959, 1961, 1962, 1977 and 1990. The epicenter of the
outbreaks in 1961 and 1962 was the Tampa area. In
1961, there were 25 cases with 7 deaths and in the
following year, there were 222 cases with 43 deaths.
One very interesting discovery made at the time was
that the SLE virus was vectored by Culex nigripalpus, a
species which had not been previously implicated in
disease transmission. In other parts of the United States,
SLE is transmitted by Culex quinquefasciatus and Culex
tarsalis. In addition to the illnesses and deaths caused
this epidemic also greatly reduced tourism business.
The reductions were estimated to be as high as $40
million, which added an enormous economic loss to the
human loss and suffering.
West Nile Encephalitis In 1999, a new
form of encephalitis was discovered in the New York
City area. Known as West Nile Encephalitis (WNE), it is
believed to have been brought in from the Middle East
by unknown means and, previous to its introduction,
had never been identified from the Western
Hemisphere. West Nile Virus (WNV) is a flavivirus that
was first isolated in 1937 from a woman in the West
Nile province of Uganda in Central Africa. WNV was first
found in the United States in 1999 during an outbreak
of the disease involving humans, birds and horses in
5

New York and New Jersey. Since then, the virus has
spread and by the end of 2004, it had been detected in
48 states and close to 30,000 human cases had been
confirmed through 2009 nationwide. WNV was first
detected in Florida in the summer of 2001 when it was
found in a dead crow in eastern Jefferson County.
Twelve human cases were reported in the State that
year. In 2002, 35 human cases of WNV illness were
detected in Florida. The peak occurred in 2003 with 99
human cases confirmed. In recent years, there have
been only a few cases annually. Since its initial WNV
activity, the virus has been reported in all 67 Florida
Counties.
Like SLEV, to which it is closely related, WNV
is maintained in a mosquito-bird cycle in nature. Culex
quinquefasciatus and Culex nigripalpus are two major
vectors of WNV in Florida. However, unlike SLE, WNV
causes high mortality in certain bird species, most
notably crows, jays, hawks and owls. It is also
pathogenic in horses. More than 1,000 cases of equine
WNV infection were confirmed in Florida from 2001-
2009.
The peak period of WNV transmission in
Florida is from July to September and most seriously
affects people older than 50 years of age. Most people
bitten by a WNV-infected mosquito will not show any
sign of illness. Of those who become clinically ill, about
20 percent will display mild symptoms including fever
and lethargy and less than 1% experiences the
neuroinvasive form of the illness. Symptoms appear
between 3 and 14 days after the bite of an infected
mosquito.
The national fatality rate has generally been 2
to 5 percent. In Florida, case fatality rates range from
4% for all cases to 7% among those who develop the
neuroinvasive form of the disease.
To prevent epidemics of encephalitis, a
surveillance program was established in the early
seventies. This surveillance includes gathering data on
cases of horses with encephalitis; checking the blood
sera of wild birds, sentinel chicken flocks, and small
mammals for the presence of encephalitis antibodies;
keeping a record of central nervous system diseases
reported from Florida hospitals; and checking
mosquitoes from certain areas of the State during the
summer and fall to screen for encephalitic viruses.
Mosquito Species in Florida
Each species of mosquito has not only certain
specific morphological characteristics, but also
physiological characteristics and habits which are
distinctive to that species. For each species, there is, for
instance, a preferential egg-laying site, a normal flight
distance/range, a preferred host animal or plant. In
addition, there is a definite temperature tolerance at
each stage of development. This range of tolerated
temperatures may be very wide or very narrow,
depending on the species. There is typically a maximum
temperature above which the animal will die, a
minimum below which it will die, and an optimum
temperature at which maximum development takes
place in a minimum of time. Both temperature and
humidity are critical for adult mosquitoes. In most
insects, the longer the optimum temperature is
maintained, the greater the number of generations the
insect may produce at a given place in a season.
Florida mosquitoes breed mainly in the
summer. Exceptions include Anopheles punctipennis,
Culex restuans and Culex salinarius, which breed all
year-round but reach peak numbers in late spring. In
north Florida, most mosquito populations are lower in
winter because of the colder temperatures, while in
south Florida, the reduced mosquito breeding
associated with winter is due to a lack of rainfall. Of the
80 species of mosquitoes found in Florida, 36 occur
throughout the State. Some of the remaining species
occur in most of the southeastern United States and the
extreme southern limit of their range falls in northwest
Florida or as far south as central Florida. Other species
which are of tropical origin cannot be found north of the
sub-tropical area of Florida - that is, the area south of a
line from Punta Gorda across to Lake Okeechobee, then
north along the coastal counties through Brevard
County (see Figure 3). A few of these species are found
only in the tropical zone, south Dade County and the
Florida Keys.
Figure 3. Fanual Zones
6

Figure 4. Mangrove Swamps Figure 5. Salt Marsh
Mosquitoes and Their Production Sites in Florida
Certain areas of Florida are characterized by
generally poor drainage. Muck, marl and other soils
perpetually saturated or subject to flooding make up nearly
half of the total land area of the State. These vast areas of
wetlands, together with thousands of grassy lake margins,
constitute an enormous potential area for mosquito
breeding.
Mosquitoes are not adapted to life in moving waters
and where they occur in flowing streams they occupy the quiet
pools and seepage areas. Aquatic environments differ chiefly in:
(1) chemistry of the waters -acid or alkaline, fresh, salt or
brackish; (2) whether natural or man-made; (3) amount of
vegetation, or type of vegetation present; and (4) whether
shady or sunny. The distinctive ovipositing habits of each
species of mosquito determine its larval habitat.
Types of Mosquito Habitats
Types of aquatic habitats are not always clearly
separate and definable, but in general they may be
classified as follows:
Salt Water or Brackish
Mangrove Swamps (Figure 4). – It is in
the transitional zone from the usual level of high tide to
levels above all but the highest spring and storm tides
that the heaviest mosquito breeding occurs, because
plant and grass cover keep moisture conditions suitable
for egg laying. Eggs are usually laid on sloping sides of
potholes, ditches, sloughs, marsh edges or on the sides
of small depressions. In some cases, however, egg-
laying occurs in extensively grass-covered level areas.
The eggs of some species require alternate flooding and
drying before hatching will occur. Species most often
occurring in these areas include:
Aedes taeniorhynchus
Aedes sollicitans
Anopheles atropos
Culex nigripalpus
Salt Marshes (Figure 5) . - North of
Daytona Beach on the east coast and north of Port
Richey on the west coast of Florida, the mangrove
swamps are largely replaced by grassy salt marshes.
Salt-tolerant herbaceous plants and typical salt grasses
dominate this type of habitat. Extensive areas are often
covered by a single species such as salt grass Distichlis
spicata, or by Batis maritima or Salicornia perennis. It is
in association with one of these plants or with black
mangrove, Avicennia nitida that breeding of the
following species occurs:
Aedes taeniorhynchus
Aedes sollicitans
7

Figure 6. Salt or Brackish ditch
Figure 7. Freshwater Marshes
Figure 8. Freshwater Lake
Salt or Brackish Ditches (Figure 6). -
The ditches which lie adjacent to salt water marshes
contain many species of grasses and support a larger
mosquito fauna including:
Aedes taeniorhynchus
Aedes sollicitans
Aedes atlanticus
Psorophora columbiae
Anopheles bradleyi
Culex pilosus
Psorophora howardii
Psorophora ciliata
Freshwater Marshes (Figure 7). - Nearly
all coastal areas have both freshwater marshes and
brackish areas, often adjacent to each other. The
shoreline along the western coast from Pasco County to
Franklin County is bordered by coastal marshes, with
little or no beach. In the Everglades, sawgrass marshes
cover more than 1.25 million acres, with Cladiurn
jamaicense the dominant low ground cover plant.
Mosquito species often found in freshwater marshes
include:
Anopheles walkeri
Anopheles crucians
Psorophora columbiae
Culex nigripalpus
Culex salinarius
Culex tarsalis
Culex erraticus
Culex peccator
Lakes (Figure 8). - There are two general
types of lakes in Florida, sand bottom and silt bottom.
Sand bottom lakes are more numerous but they do not
afford as many mosquito habitats as the silt bottom
lakes. Vegetation, usually composed of emergent
grasses, occurs only in a narrow band along the margin
and larvae are confined to this littoral zone. Silt bottom
lakes are frequently bordered by cypress trees and
many species of floating or emergent plants. The lake
bottom consists of a layer of organic detritus made up of
decaying vegetation and the lake usually has a fairly
heavy cover of vegetation composed of such plants as
water hyacinths or bonnets. Mosquito larvae are more
common near shore but may be found throughout the
lake wherever cover is afforded. Species likely to be
found in lakes and marshy areas around lakes include:
Anopheles smaragdinus
Anopheles crucians
Anopheles quadrimaculatus
8

Anopheles walkeri
Uranotaenia sapphirina
Uranotaenia lowii
Culex salinarius
Culex nigripalpus
Culex erraticus
Culex peccator
Coquillettidia perturbans
Mansonia dyari
Mansonia titillans
Ponds and Seepage Areas (Figure 9). -
There is no clear distinction between a pond and a lake
except that ponds are generally smaller. Grassy
woodland ponds or fluctuating ponds occupy shallow
depressions and are filled by rainwater or surface run-
off. They are usually of uniform depth but the area they
cover will vary, depending on rainfall. Sinkhole ponds
are usually quite deep and may be covered with
vegetation or free of all except marginal plants. Both
these types of ponds may contain larvae of:
Anopheles crucians
Anopheles quadrimaculatus
Culiseta inornata
Culiseta melanura
Culex nigripalpus
Culex quinquefasciatus
Culex restuans
Culex salinarius
Culex erraticus
Culex peccator
Culex pilosus
Culex territans
Aedes canadensis canadensis
The seepage areas around hillsides and ponds or
streams most often breed:
Anopheles punctipennis
Anopheles georgianus
Anopheles quadrimaculatus
Aedes sticticus
Psorophora ferox
Springs (Figure 10). - Mosquito breeding in
springs is restricted to the quiet edges where vegetation
affords cover for the larvae and there is little if any
water movement. The only species recorded from this
habitat in Florida are:
Anopheles quadrimaculatus
Anopheles perplexens
Figure 9. Ponds and Seepage Areas
Figure 10. Springs
9

Swamps (Figure 11). - Swamps differ from
marshes principally in having a more dense cover made
up of larger trees such as cypress, red maple, and
tupelo. The most common species of mosquito larvae
found in swamps are:
Anopheles smaragdinus
Anopheles maverlius
Anopheles inundatus
Anopheles diluvialis
Anopheles crucians
Anopheles quadrimaculatus
Culiseta melanura
Aedes canadensis
Mansonia species
Coquillettidia perturbans
Borrow Pits and Canals (Figure 12)
. - These
man-made bodies of open water produce more
Figure 11. Swamps
mosquitoes as they silt-in and become overgrown with
vegetation. They yield this variety of species:
Anopheles maverlius
Anopheles quadrimaculatus
Culiseta inornata
Psorophora columbiae
Aedes canadensis
Culex nigripalpus
Culex quinquefasciatus
Culex restuans
Culex salinarius
Anopheles albimanus
Coquillettidia perturbans
Mansonia species
Specific Aquatic Plant Associations (Figure
13). - Species of mosquitoes found in association with
specific aquatic plants are:
Coquillettidia perturbans
Mansonia dyari
Mansonia titillans
Bromeliads and pitcher plants
Wyeomyia vanduzeei
Figure 12. Borrow Pits and Canals
Wyeomyia mitchellii
Wyeomyia haynei
Culex biscaynesis
10

11
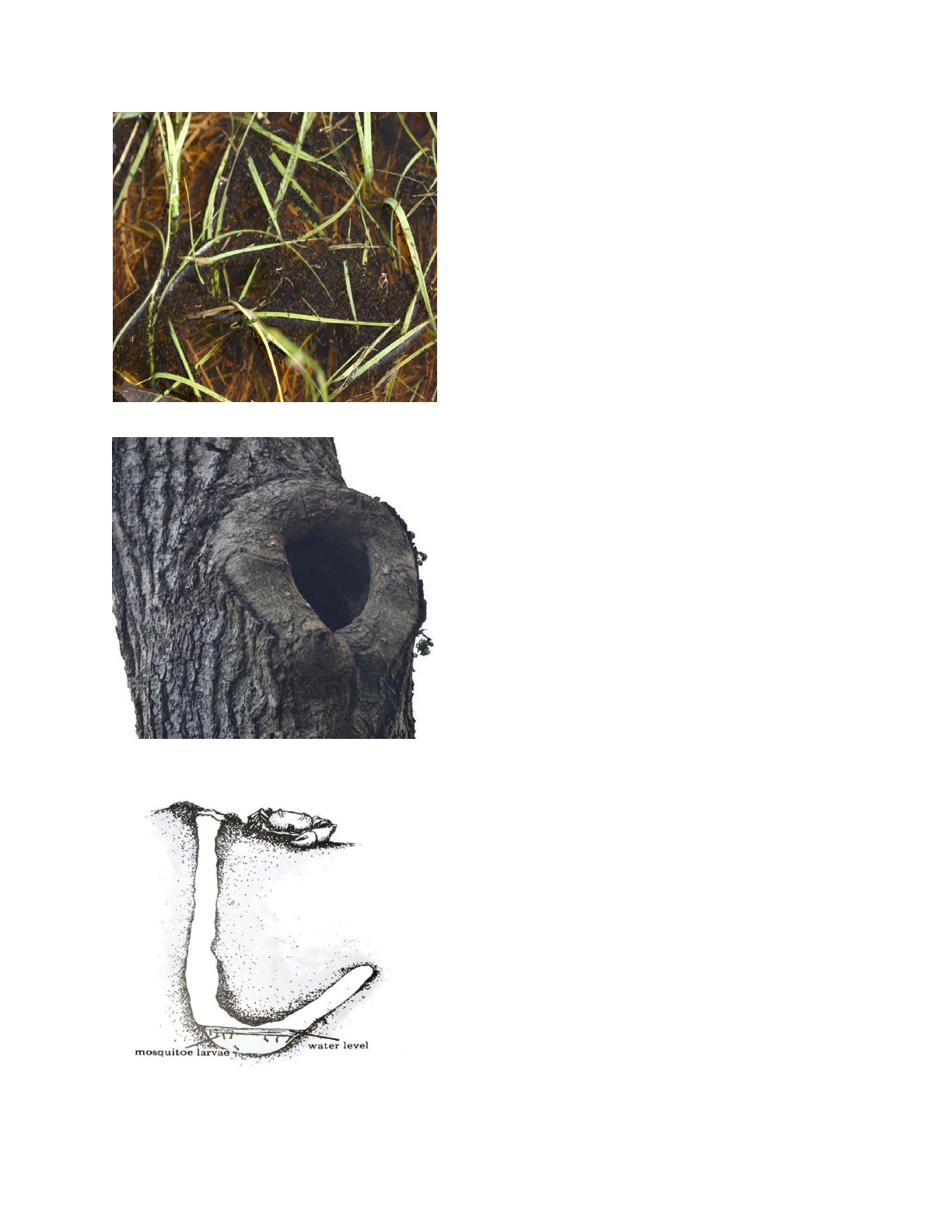
Figure 14. Rain and Flood Water Pool
Figure 15. Tree Holes
Figure 16. Land Crab Holes
Rain and Floodwater Pools (Figure 14). -
These transient pools form the breeding place for a
large number of species, especially among the
Psorophora and Aedes. The pools disappear in dry
weather and support no true aquatic vegetation, though
there is usually a layer of leaves and other detritus
settled on the bottom. Mosquito species found in this
habitat are:
Psorophora johnstonii
Psorophora pygmaea
Aedes atlanticus
Aedes dupreei
Aedes fulvus pallens
Aedes infirmatus
Aedes mitchellae
Aedes sticticus
Aedes tormenter
Aedes vexans
Aedes cinereus
Culex atratus
Culex pilosus
Culex bahamensis
Culex nigripalpus
Tree Holes (Figure 15). - Tree holes or rot
cavities support a rather extensive and unusual
mosquito fauna, with many species breeding almost
exclusively in this habitat. They are:
Anopheles barberi
Toxorhynchites rutilis rutilis
Toxorhynchites rutilis septentrionalis
Aedes triseriatus
Aedes hendersoni
Orthopodomyia sianifera
Orthopodomyia alba
Aedes thibaulti
Aedes albopictus
Crab holes (Figure 16). - Along the eastern
coast of Florida south of St. Johns County the holes of
the large land crab, Cardisorna guanhumi , serve as
larval habitat for:
Deinocerites cancer
Culex opisthopus
12

Freshwater Drainage Ditches (Figure 17). -
Freshwater ditches in pastures, at the bottom of road
shoulders, in old fields, and in lowland groves will often
yield the following species of mosquito larvae:
Psorophora columbiae
Culex nigripalpus
Culex pilosus
Culex erraticus
Culex quinquefasciatus
Anopheles crucians
Anopheles walkeri
Aedes atlanticus
Uranotaenia sapphirina
Uranotaenia lowii
Psorophora ciliata
Aedes sollicitans
Figure 17. Freshwater Ditch
Artificial Containers (Figure 18). - Several
species breed in man-made situations around human
dwellings. Tin cans, fish pools, rain barrels, bird baths,
and old tires containing water serve as the larval
habitat. Species most often encountered are:
Aedes aegypti
Aedes triseriatus
Culex quinquefasciatus
Culex restuans
Culex salinarius
Culex nigripalpus
Anopheles quadrimaculatus
Aedes albopictus
Figure 18. Artificial Containers
13

Identification
Mosquitoes can be collected as either larvae or
as adults and many species can be identified in either
life phase. It is important to determine what species are
present and their relative abundance so that mosquito
control personnel will know what their problem
mosquitoes are and where they are breeding. Only in
this way can they most efficiently use the control tools
available. Every person who works in mosquito control
should be able to recognize the common problem
species in their area.
All mosquito species in Florida fall into one of
these subfamilies: Toxorhynchitinae (genus
Toxorhynchites); Anophelinae (genus Anopheles); or
Culicinae (the other ten genera).
Figure19. Fourth Stage of Anopheles and Culex Larvae
14

Figure 20. Characteristics of Anophelines and Culicines
15

The larvae of Toxorhynchitis are found in tree
holes or artificial containers. They are very large and
predacious, feeding on such mosquito larvae and other
small animals as they occur in their breeding place.
They have an almost square head and the hairs on the
thorax and abdomen arise from heavily chitinized
plates. The females do not take blood as adult
mosquitoes, but feed only on plant nectar and juices.
Anopheline larvae (Figure 19) are
characterized by the absence of a siphon, and the
presence of a palmate (palmetto-shaped) hair dorsally
on each side of, at least, segments IV-VI of the abdomen.
Anopheline larvae usually lie parallel to the surface of
the water.
Culicine larvae always have a siphon (Figure
19) which may or may not bear a pecten, a row of
spines. They do not have palmate hairs. These larvae
usually lie with the head downward at a 45 degree
angle to the water surface.
With practice it may be possible to identify
some species as adults or as fourth instar larvae with
the unaided eye or a hand lens. However, because it is
easy to misidentify in the field, samples should be taken
into the laboratory to be verified under a microscope. A
stereoscopic microscope to be used for adult and larval
identification should have a magnification range of 10X
to 40X, the lower power for use in sorting specimens
that are readily identifiable and the higher power for
detail work. Specific identification of difficult larval
characteristics or male terminalia may require
magnifications of up to 400X.
Larval Morphology
The characters used in the identification of
genera of mosquitoes found in Florida are clearly
labeled in Figure 19. By studying these illustrations it
will be possible to key fourth instar larvae to genus,
using Figure 22.
Adult Morphology
The external anatomy of an adult female
mosquito is shown in Figure 21. The Pictorial Key to the
12 genera found in Florida (Figure 23) makes it possible
to identify females to genus by comparing distinctive
features. You simply follow the character in each pair
which fits the specimen you are identifying, following
the lines down until you reach the correct choice which
names the genus.
Some Problem Species of Mosquitoes in Florida
Common Problem Mosquitoes
The primary pest mosquitoes in Florida are
the salt marsh species, Aedes taeniorhynchus and Ae.
sollicitans. Ae. taeniorhynchus is a small black and white
mosquito with distinct narrow white rings on the tarsi
and on the proboscis. Wing scales are all dark. Ae.
taeniorhynchus is the predominant species, produced in
huge numbers, all around the coast of Florida.
Eggs are usually deposited on damp soil where
ground vegetation is thick. Sod samples have yielded up
to 100 million eggs per acre. The larval embryo is fully
developed in about three days and is ready for hatching
as soon as it is flooded by the tides or rainfall. The
longer the period is before hatching, the greater the
chance of the embryo dying, although some of the eggs
will hatch after many months.
The length of time passed as a larva, before
pupation, depends on temperature and available food,
and ranges from four days to four weeks. The pupal
stage may last from 30 hours to several days, depending
on temperature. Emergence from a breeding area may
go on for several days. Mating may occur during the
general flight activity of a newly hatched brood. The
adult rests for at least six to eight hours and after dark,
a large number will migrate, flying as far as 25 miles,
usually downwind and parallel to the coast. Migration
may be repeated on a second or third night and then the
brood settle down to feed, rest, and lay eggs. Adults feed
on nectar as an energy source.
A blood meal, taken only by females, serves as
a source of protein for egg production, although some
Ae. taeniorhynchus are capable of laying eggs without
the first blood meal, by utilizing protein carried over
16

from the larval stage. This species is active chiefly after
sunset. During the day the mosquitoes rest on the
ground where grass or leaves offer a dark, moist, cool
hiding place. However, if a stimulus reaches them, they
will fly to it. It is not uncommon that if you go where
they are in the daytime, they will be stimulated to bite
you.
Aedes sollicitans occurs around the entire coast
of Florida, but is more common in the northern half of
the State. In localized situations, it may outnumber Ae.
taeniorhynchus. Ae. sollicitans is somewhat larger than
Ae. taeniorhynchus and is more golden brown with
wider, pale bands on tarsi and proboscis. The wing
scales are mixed light and dark. Each abdominal
segment has a median longitudinal band of pale scales
in addition to the pale basal transverse band. This
species has a life history similar to that of Ae.
taeniorhynchus, breeding in the salt marsh, but the
larvae have also been found in great numbers in coastal
swales and inland in brackish waters. The adults usually
rest during the day, but the females are persistent biters
and will attack at any time of night or day.
The exact seasonal distribution of the salt
marsh species is dependent on the tides and on rainfall,
but usually each year they begin to emerge in large
numbers in May and continue through October.
The other main problem species in Florida
include the flood-water species (Psorophora columbiae,
Ps. ferox, Aedes atlanticus, Ae. infirmatus, and
Ae. mitchellae) which breed in intermittently flooded
areas of fresh water, as well as Culex nigripalpus, Cx.
quinquefasciatus and Cx. salinarius, which usually breed
in more permanent fresh water habitats such as ponds
17
and ditches. In many areas of Florida, Coquillettidia
perturbans emerges in enormous numbers, and in
central and south Florida, Mansonia dyari is a serious
pest. In the spring, Aedes canadensis and Ae. sticticus
emerge in large numbers in northwest Florida, although
they are comparatively rare in the rest of the state.
Other Problem Mosquitoes
Aedes aegypti is a small, dark, mosquito easily
recognized by the silvery-white lyre-shaped marking on
the thorax and the silvery-white bands on the tarsi.
Historically, it was one of the most common domestic
mosquitoes, laying its eggs on the sides of containers
such as tin cans, tires, vases, small pools, tree holes and
yard plantings of certain bromeliads. Its numbers,
however, have been drastically reduced in north and
central Florida by, as yet, unknown factors related to
the recent introduction of Aedes albopictus, (see
narrative of Aedes albopictus below). The embryos
develop in two to four days and will hatch when
flooded. The cycle from egg to adult may be completed
in 10 days in warm weather.
The adults feed warily, often biting the ankles.
They never fly more than a few hundred feet from the
emergence site. Because this mosquito is the vector for
both yellow fever and dengue fever, campaigns have
been instituted in various countries of this hemisphere
to eradicate the species, including a project within the
last three decades to eliminate them in this state. The
project was discontinued, however, before completion
and Ae. aegypti became at least as common, if not more
numerous, than before the eradication project.

Figure 22. Pictorial Key to U.S. Genera of Mosquito Larvae
18

Figure 23. Pictorial Key to U.S. Genera of Female Mosquitoes
19

Aedes albopictus, "the Asian Tiger Mosquito",
was introduced from Asia into Florida in 1986 and has
expanded its range to every part of the State but the
middle and lower keys. In northern and central Florida,
Ae. albopictus is replacing the related species, Aedes
aegypti, in areas where the two mosquitoes share
breeding sites. Similar to Ae. aegypti in size, appearance,
and habits, this mosquito can be identified by the single,
silver, longitudinal line on the thorax and by the
strongly contrasting silver and jet black body
coloration. An aggressive daytime biter, Ae. albopictus is
considered a major vector of dengue in Asia. While
dengue has disappeared from Florida for many years,
the recent introduction of this mosquito into the U.S.
has some officials concerned about the increased
potential for epidemics of this viral disease.
The larvae of Aedes triseriatus are usually
found in water collected in rot cavities of trees, although
they frequently occur in artificial containers along with
Ae. aegypti, and Ae. albopictus. The adult is dark with a
conspicuous area of white shiny scales on each side of
the thorax. Near their breeding place these mosquitoes
will attack man during the day or early evening and
their bite is painful and lasting.
Aedes mitchellae is similar in appearance to Ae.
taeniorhynchus in being black with pale rings on the
proboscis and tarsi. It differs in having the femora and
tibiae speckled with pale scales and in having a
longitudinal stripe or patches of pale scales on the
abdomen in addition to the pale basal abdominal bands
on each segment. It breeds in stump holes and flood-
water pools. Ae. mitchellae is a severe biter, common in
the northern and panhandle areas of Florida.
Aedes atlanticus is a dark, medium-sized,
species which has a distinct median pale stripe running
the length of the thorax. This mosquito lays its eggs on
damp soil and the larvae develop in the shallow pools
following rainfall. The adults bite readily, even in
sunlight. It is often found in association with Ae.
infirmatus, which has a broader pale stripe that extends
only about two-thirds the way back on the thorax. This
species bites readily.
Aedes canadensis canadensis, which has pale
rings both at the base and tip of the tarsal segments, is a
common nuisance flood-water mosquito in the northern
section of Florida. Aedes vexans, distinguished by its
very narrow pale tarsal bands and by basal abdominal
bands which are notched medially on the posterior
border, is common throughout most of the state. It
usually feeds in shady places during the day, but is often
particularly annoying at dusk and after dark. The larvae
are often found in large numbers in irrigated groves.
Psorophora mosquitoes commonly breed in
flood-water and include Ps. ciliata, a very large shaggy
black and yellow species commonly called the "feather-
legged gallinipper". Ps. ferox is a smaller purplish
mosquito with conspicuously white tips on the hind legs
(tarsal segments 5, 4 and part of 3); and Ps. Columbiae is
a large black and white species distinguished by a pale
subapical ring on each femur. Psorophora columbiae is
20
one of the most troublesome pests in Florida. It will bite
viciously any time of the day or night, but is especially
active at night. It has been known to feed in such
numbers in the everglades that cattle were lulled by
loss of blood and suffocation. The adults emerge in huge
numbers from improved pastures and irrigated groves
and from woodland pools, roadside ditches, and swales.
There are three main problem Anopheles
mosquitoes in Florida. Anopheles crucians adults have
distinct areas of pale scales on the wing. This species
breeds chiefly in the slightly acidic waters of cypress
swamps and in ponds and lakes. It has been found
naturally infected with malaria, but is not considered an
important vector of the disease since it apparently
prefers to feed on large mammals rather than man.
Anopheles quadrimaculatus is the most
common and widespread member of a larger species
complex consisting of 5 morphologically distinct but
similar species. Although very similar in appearance,
they can be separated with great care and differ
somewhat in their preferred habitat and range.
Anopheles quadrimaculatus breeds mostly in stagnant
alkaline fresh water which has emergent or floating
vegetation or debris. It was the primary vector of
malaria in the southeastern United States. The adults
are characterized by having four, more or less, distinct
spots on the wings. They feed actively on man and
animals, chiefly at night or sometimes in the day in dark
areas in and around buildings. There may be as many as
10 generations in a season.
Anopheles atropos larvae are found in
permanent brackish to salt pools and marshes. The
adults, entirely brownish black, will attack man readily,
even in bright sunlight. The species is not considered a
disease vector.
Culiseta inornata, a very large species
breeding in pools, ditches and occasionally in artificial
containers, is primarily a late fall and winter breeder in
Florida. The adults apparently prefer to feed on
livestock, but also will attack man.
Culiseta melanura, a smaller, very dark
species, breeds in small permanent bodies of water,
particularly in freshwater swamps. Females feed chiefly
on birds and the species is considered to be the primary
vector of Eastern Equine Encephalitis from bird to bird.
Coquillettidia perturbans is the most common
and wide-ranging of the mosquitoes whose larvae
breathe by piercing the roots or stems of aquatic plants
with their siphon. This species has been identified in
every county in Florida. Many aquatic plants may serve
as host to this species, including water lettuce, water
hyacinths, and cattails. Although the females usually
feed at night, they have been known to feed on man
during the day in shady areas where they are resting.
This species is suspected of being an important
secondary vector of EEE to horses and man. Cq.
perturbans is a fairly large species with a golden brown
coloration, while the other two species are smaller,
darker, and are very difficult to distinguish from each
other. Mansonia titillans larvae also attach to a number

of different aquatic plants, but Ma. dyari in Florida has
been found associated primarily with water lettuce.
The Culex mosquitoes all breed in fresh water
habitats such as pools, ditches, and ponds. Culex
quinquefasciatus larvae are often associated with foul
water such as effluents of sewage treatment plants,
which have been found producing these mosquitoes by
the thousands. The larvae are also taken in catch basins,
cesspools, polluted ditches and ponds, and in containers
holding water in homes and around buildings. The
adults are distinguished by having a pale basal band on
each abdominal segment rounded on the apical margin
so that the band is wider in the middle and narrower on
each side. The females are said to show a preference for
bird blood, but they often get into homes and feed
readily on man at night. In some areas of the country,
this species is the primary vector of St. Louis
Encephalitis (SLE).
Culex salinarius larvae are often found
associated with Cx. nigripalpus larvae, and have been
collected occasionally from small ground depressions
and stump holes. Emergences are concentrated in the
cooler months. The females will bite readily outdoors
and sometimes enter buildings to feed on man. The
species is characterized by golden scaling on the entire
seventh abdominal segment.
Culex nigripalpus is a small black mosquito
with white lateral abdominal patches. It breeds in
permanent or semi-permanent waters where there is an
abundance of decaying leaves and vegetation. Larvae
have also been found in brackish water. This species
usually bites outdoors. It was formerly believed to be of
little medical importance, but during the St. Louis
Encephalitis epidemic in the Tampa Bay area in 1961
and 1962, it proved to be a primary vector of the
disease. Since that time extensive studies of the life
history of this mosquito have been carried out at the
Florida Medical Entomology Laboratory at Vero Beach.
This mosquito is readily taken in light traps.
Culex restuans larvae occur in a variety of
freshwater habitats. In Florida, adults appear primarily
during cooler weather. Females will sometimes come
into homes and bite after dark, but they are not a
primary nuisance, preferring birds to humans. The adult
is similar to Cx. quinquefasciatus except that the
abdominal bands are straight on the apical margin and
the thorax often has four small patches (spots) of pale
scales.
In contrast to these previously mentioned
species, some species of mosquitoes are not a big
problem, but may be extremely annoying in local areas
where they breed. For instance, Deinocerites cancer;
which breeds almost exclusively in water collected in
land crab holes, will bite humans who come to their
breeding habitat. Three species of Wyeomyia, small
mosquitoes which breed in water collected in plants,
occur in Florida. One of these, Wy. vanduzeei, which
breeds in bromeliads, will feed and be very annoying if
humans come into their vicinity.
Mosquito Control Practices
Responsibilities of a Mosquito Control
Director
The qualifications for a mosquito control director,
depending on the size of the local budget for mosquito
control, are set out in the Mosquito Control Rules,
Chapter 5E-13, F.A.C.. It is the duty of the director to
plan, supervise, and direct the execution of the county
or district arthropod control program. This makes the
director responsible for every aspect of the working
program, including:
1) Determining the extent of the problem and
locating the breeding areas.
2) Planning appropriate projects and controls to
alleviate the problems.
3) Preparing and submitting for approval the
monthly reports as required by Chapter 5E-13,
F.A.C.
4) Purchasing equipment and materials,
providing for maintenance, and maintaining
inventory records.
5) Hiring and assigning necessary personnel.
6) Seeing that all work is carried out in a safe,
effective and efficient manner in compliance
with the Federal, state, and local laws and all
regulations pertaining to mosquito control.
7) Evaluating the results the program achieves
and providing for surveillance of breeding
conditions in the county or district.
8) Establishing good public relations for
mosquito control.
9) Continually improving his knowledge and
abilities through local and national
associations, meetings and publications.
A mosquito control director must be able to
depend on the abilities and integrity of his supervisors
and equipment operators. The supervisor of a crew
operating heavy equipment or applying insecticides
must give his crew clear and complete instructions,
must see that all safety precautions are adhered to, and
that all equipment is kept in good working condition.
In the final analysis, the success of a program
often depends on the correct application of insecticides,
on the ability and willingness of the applicator to use
the materials and equipment as instructed and to
immediately report malfunction of equipment. This
ensures the correct dosage is applied without
endangering the applicator, the public or the
environment. It is important for every ground
equipment operator and pilot to know how to safely use
his equipment, how to calibrate and check it, and how to
maintain it. Accurate record keeping is an essential for
21

evaluating the effectiveness and efficiency of insecticide
adulticiding.
Continuing Education
In order to do the best possible job in any field,
it is necessary that employees know of new methods
and materials that can help them to better accomplish
their purpose. Each new employee should be fully
trained for his job -what he is expected to do, how he is
to do it, and why. It is good practice to have refresher
and updating courses on insecticide usage and safety
practices for all employees. This is especially important
for employees holding PHPC certifications, as this
license is renewed through the accrual of 16 hours of
continuing education every 4 years.
The director of the program should keep up
with new developments in mosquito control through
reading technical journals and pamphlets, by talking
with representatives of equipment and chemical
companies, and by belonging to and attending meetings
of associations in his field. One of the most useful
journals for directors is the Journal of the American
Mosquito Control Association (AMCA). Annual meetings
of the AMCA and the Florida Mosquito Control
association (FMCA) will also prove helpful, both as a
source of new ideas and for an exchange of information
and ideas with other directors.
Planning the Project
Before any control effort is made, the director
must know the extent of the problem in his area. He
must know what species are involved, the level of
annoyance from mosquitoes, and the location of
breeding areas. Even after the initial survey, routine
checking (surveillance) will be needed because of
seasonal variations in the fauna, because of changes in
the topography, and as a means of evaluating how the
projects are progressing.
To identify the problem, larvae and adults
should be collected throughout the area. To ensure
effective control, it is very important to be able to
identify the location for each collection. Collecting sites
may be identified by an address, such as "fish pond at
634 Lane Avenue", by description such as "in pasture
pond at intersection of State Road 84 and U.S. 1", or by
using a map or GIS coordinates. Additional data on the
collection site such as a list of dominant vegetation or
evidence of gross pollution is useful. Larval collections
are usually made with a long-handled dipper and counts
are based on the number of larvae per dip. The larvae
are usually preserved in alcohol for later identification
in the laboratory.
In marshes, larval dipping is sometimes done
from a hovering helicopter, making it possible to check
breeding areas not otherwise accessible to the
inspector.
Adult mosquito surveys are most often made
using light traps. The New Jersey trap is operated using
a standard household current and is a good choice when
convenience and long-term monitoring from a
permanent site are important. New Jersey traps,
however, tend to also collect larger organisms, i.e.
beetles, moths and frogs, which can damage the
collection and make identification difficult (Figure 24).
The CDC miniature light trap, (Figure 24) baited with
dry ice to release carbon dioxide will usually capture
much larger numbers of mosquitoes and may attract
some species which do not usually come to the New
Jersey trap in significant numbers. CDC traps are
compact and highly portable but are operated by
batteries which need fairly frequent recharging or
replacing. It is important to note that traps are selective
and only give an indication of what species are present
and their relative abundance.
Figure 24. CDC miniature light trap (left) and New Jersey light trap (right)
22

Other methods of judging the extent of the mosquito
problem include landing rate counts -the number of
mosquitoes which land per minute -and collecting by
aspirator in fixed resting stations such as culverts,
sheds or houses. The number of telephone complaints
received by the mosquito control office is also an index
of the magnitude of the problem, but should be relied
upon only when followed up by inspection or when
taken from individuals who have a proven history of
reliability.
In locating breeding areas and in planning
source reduction projects, the director must have
accurate knowledge of the topography of his district.
For example, his program must be aware of the size and
position of streams, lakes and roads and the elevation
throughout the area. In addition, he will want to know
the location of recreational areas, wildlife reserves,
state and national parks, large bridges, towers and
power lines. Among the maps which will be especially
useful are: shaded relief maps, road maps, population
maps, soil maps, drainage maps, and aerial
photographs. Plans for engineering projects for
mosquito control can be shown as map overlays, and
areas to be sprayed by plane can be marked on the
maps for the pilot's use.
Figure 25. Comparing ULV (left) and Thermal Fogging (right)
Equipment for Mosquito Control
Each mosquito control district is different and
will need a different combination of vehicles and other
equipment.
Larviciding Equipment - One of the oldest methods
of mechanical application of larvicides is by
knapsack/backpack sprayer or by using a hand-
operated granular applicator. In the interest of covering
a larger area more quickly, manual application has been
largely replaced by more mechanized methods.
However, the knapsack sprayer is still often used in
urban areas, along drainage ditches and in catch basins
where it is desirable to make a very localized larvicide
application. With the exception of applications made to
roadside ditches and other areas readily accessible to
ground vehicles (i.e. trucks), larviciding of large areas is
usually done by making applications from airplanes and
helicopters.
Adulticiding Equipment - Control of adult
mosquitoes is usually accomplished through fogging,
spraying, or by ultra-low volume (ULV) spraying.
Mosquito control districts in Florida may own a variety
of vehicles and equipment such as: cars, station wagons,
jeeps, fog trucks, tractors, draglines, bulldozers,
backhoes, pick-up trucks, airplanes, and helicopters.
23

Tractors, bulldozers, and backhoes are used in
diking, filling, and impounding, as well as in operating a
sanitary landfill in such a way that it does not breed
flies or mosquitoes. This type of control activity can be
considered habitat reduction.
A variety of fogging and spraying equipment is
available and includes mist blowers, "cold foggers",
thermal fog generators, and ULV machines.
Aircraft equipped for conventional spraying,
or adapted for ULV applications are widely used
throughout the State, both for larviciding and
adulticiding. Helicopters are often used both for
larviciding and adulticiding and may be used for both
larval surveys and for applying larvicides. However,
fixed-wing aircraft, both single and multi-engine, are the
aircraft most commonly used by the control districts for
both adulticiding and larviciding. Use of fixed-wing
aircraft is the most efficient means to adequately treat
large areas of land.
Calibration of ULV Machines and
Checking Droplet Size
ULV application of pesticides is a method
whereby the insecticide, usually a technical or undiluted
material, is broken up into very small droplets. Most
equipment uses the air blast of a blower to break up the
droplets and transport them away from the vehicle, but
some machines use other methods to produce and move
the small droplets. The primary reason a piece of
equipment must be calibrated is to make sure it is
operating in an effective manner and discharging the
insecticide in the correct amounts according to label
recommendations of the particular insecticide.
The calibration of ULV equipment is a
relatively simple process since it requires a minimum
amount of equipment. A timepiece, preferably a stop
watch, and two containers (one to collect the insecticide
and one for measuring) should be sufficient to measure
insecticide flow. Obviously, when discharging only ½ to
4 fl. Oz/min (15 to 125 ml/min) as with ULV sprayers, a
measuring container calibrated for small amounts is
required. A glass container marked in milliliters (ml) or
tenths of a fluid ounce is ideal.
To calibrate ULV equipment, first, disconnect
the insecticide line from the nozzle and place the tip of
the line in a container to collect the discharge. Start the
machine and when it is operating at the desired
pressure, etc., set the flow meter or digital readout
about mid-scale of where you think it should be for the
desired discharge. While the material is being
discharged into the collection container, move the
discharge line to the calibrated measuring container for
a predetermined time, usually 1min. At the end of that
time, move the discharge line back to the collection
container and record the amount that was discharged
into the measuring container. If the discharge is too
much, reduce the setting and repeat the procedure; if it
is too little, increase the setting. Repeat the entire
procedure as many times as necessary until the
24
permanent mosquito control projects such as ditching,
machine is dispensing the recommended volume per
minute. Repeat at the same setting as a check. If the
discharge is satisfactory, reconnect the insecticide line
to the nozzle. The recommended discharge in fl. oz/min
for a particular insecticide is shown on the insecticide
label.
If the machine is equipped with the older ball
type flow meter control system, the temperature of the
insecticide at the time of calibration should be noted
since the amount of material being discharged at a
particular flow meter setting will vary according to the
temperature of the insecticide. If the temperature in
actual operation is less than when calibrated, the
discharge will be less and in order to discharge the
correct amount of insecticide, the flow meter setting
will have to be increased. For example, when spraying
malathion with the Leco generator, a 5°F difference in
temperature will result in a 1/2 fl. oz. difference in
discharge. Therefore, when discharging 2 fl. oz/min,
there is an unacceptable 25% error in discharge.
Variations in temperature do not affect all insecticides
equally. Some equipment manufacturers offer tables or
curves which indicate the flow meter setting for several
insecticides at various temperatures and discharge
rates. In machines which have positive displacement
pumps, such as the variable flow and constant flow
control systems, insecticide temperature is not a factor.
The insecticidal distribution system of the ULV
machine should be flushed with approximately one pint
of isopropyl alcohol following each time the unit is used.
Once a ULV machine has been calibrated to
deliver the correct dosage of an insecticide, it is
necessary to determine whether the insecticide is being
dispersed in the correct droplet sizes. Instructions for
testing droplet size are given on some insecticide labels.
Recent improvements in testing for droplet
size include the use of a stand with a wooden arm to
which slides are attached. The arm is dropped through
the insecticide coming from the machine. This
mechanism gives a more uniform deposition rate than
waving the slides by hand; however, it works only with
machines that use a blower to propel the droplets from
the nozzle.
Since droplet size varies with flow rate,
different formulations, and formulation pressure, as
well as, to some extent, with temperature, it is
important to check droplet size frequently. It is
recommended that droplet size be checked each time
the unit is put into service following repairs or
maintenance. The droplet size should be verified every
100 hours of operation or as often as necessary to
ensure it is producing droplets in the required range.
Calibration of Thermal Fog Equipment - Since
thermal foggers discharge much greater volumes than
ULV equipment, a larger measuring container must be
used. Because of the low viscosity of the dilute
insecticide solution, the temperature of the solution is
not a factor in determining discharge rates.

Maintenance of Equipment - The importance of
proper maintenance cannot be overemphasized.
Machine breakdown is both annoying and expensive.
Because timing is often of great importance in adult
mosquito control, a machine failure can completely
destroy the value of any specific operation. An
instruction manual and a parts manual should be
available for each piece of equipment and they should
be kept at hand. Both the machine operator and his
supervisor should be familiar with their contents.
Methods of Mosquito Control
Premises Sanitation
The need to prevent mosquito breeding in
water holding containers around homes and businesses
is well known, but unfortunately has not received much
emphasis in recent years. Each mosquito control
director should use the media available to him to
educate the general public in the need to see that jars,
cans, old tires and other junk, bird baths and water-
holding plants do not breed mosquitoes. Removing
these items or dumping any water in them is a simple
step that can be taken to help combat certain species of
mosquito.
Land and Water Management
Land and water management methods do, in
many instances, alter the environment and are,
therefore, subject to the environmental permitting
process. In the past, ditching in the salt marshes to
provide water circulation and to make the marshes
available to fish which feed on mosquito larvae has been
widely and successfully carried out in Florida. Another
effective method of salt marsh mosquito control has
been diking and creating an impoundment which covers
the surface of the marsh with shallow water and
prevents salt marsh mosquitoes from laying eggs, since
they are laid on damp soil and not on water.
Unless specifically exempt, most dredging and
filling activities require permits if the activity is to be in
"submerged lands or the transitional zone of submerged
lands" as defined by the vegetation indices listed in
Chapter 17-4, Florida Administrative Code.
The application for a permit is submitted to
the Department of Environmental Protection who in
turn sends copies to other state agencies and the U.S.
Army Corps of Engineers. The applicable water
management district should also be contacted to
determine if a permit from them is required. A local
permit is not usually needed, but this should be
investigated.
Existing projects which need maintenance
may be exempt from the permitting process, especially
if the spoil is to be placed on an upland site as defined in
Chapter 17- 4, F.A.C.
The Department of Agriculture and Consumer
Services, Bureau of Scientific Evaluation and Technical
Assistance, will assist mosquito control districts in
developing permit applications so that water
management work may remain an essential element of
mosquito control programs.
Chemical Control
Throughout the world the chemical control of
mosquitoes has significantly reduced human illness and
death, and has greatly improved human comfort by
rapidly and effectively reducing vector species and pest
populations. Although the use of chemical materials has
been a publicly sensitive issue, chemical insecticides
have been responsible not only for creating a healthier
environment for human beings, but also for making it
possible to develop and utilize land areas previously
considered unfit for human habitation.
Chemical insecticides are used in Florida both
as larvicides and as adulticides. With certain exceptions,
no chemicals may legally be used for these purposes
unless they have been approved by the Environmental
Protection Agency (EPA) and registered by the Florida
Department of Agriculture and Consumer Services.
Larvicides
Three categories of larvicides are used
extensively for larval control in Florida. These include
contact larvicides (certain organophosphate and
hormone mimics), surface control agents (surface oils
and films), and stomach toxins (microbial larvicides).
Temephos belongs to the class of insecticides
known as organophosphates (OP). Temephos is
currently the only OP registered for use as a larvicide in
Florida. Like the other OPs, the mode of action is to
inhibit cholinesterase in the peripheral and central
nervous systems of the larval mosquitoes. Temephos
has a relatively low to moderate acute toxicity
compared to other organophosphate insecticides.
Registered formulation types containing temephos
include granular and emulsifiable concentrates. Product
labels typically bear either the signal word “WARNING”
or the signal word “CAUTION”, indicating they are of
lower irritancy or toxicity. Temephos products are
labeled for use in many habitats including tidal
marshes, woodland pools, polluted water, tires, and as a
pre-hatch treatment.
Methoprene is a juvenile hormone (JH)
analog which can be used as a larvicide, since it can
regulate insect growth. Methoprene will not control
adult insects. Juvenile hormone must be absent for a
pupa to molt to an adult. Methoprene effectively inhibits
the transformation of a pupa to the adult insect. It is
considered a biochemical pesticide because rather than
controlling mosquito larvae through direct toxicity,
25

methoprene interferes with an insect’s life cycle and
prevents it from reaching maturity or reproducing.
Therefore, EPA lists methoprene as a biopesticide, and
its labels bear the signal word “Caution”.
Larviciding Oils form a coating on the top of
the water and drown larvae, pupae, and emerging adult
mosquitoes. Surface oils are considered one of the most
effective tools for pupal control and can control newly
emerged adults that are resting on the water surface
when drying their wings. Over all, they have a low
toxicity when used according to the label with minimal
detrimental effects to non-target organisms. EPA has
also assigned larviciding oils a “CAUTION” signal.
Monomolecular surface films such as
Arosurf MSF and Agnique MMF are utilized as larvicides
and pupicides of mosquitoes. They are biodegradable
and spread spontaneously over the surface of the water
to form an ultra-thin film. Their mode of action is
physical rather than chemical. These compounds lower
the water surface tension, preventing suspension of the
larvae and pupae at the water surface, subsequently
suffocating them. They also interfere with emergence of
the adults. Monomolecular films, used according to label
directions for larva and pupa control, pose minimal
risks to the environment and human health. Because
they do not last very long in the environment, they are
usually applied only to standing water. Typical sites of
application include roadside ditches, woodland pools,
or containers which contain few non-target organisms.
Bacillus thuringiensis israelensis (Bti) and
Bacillus sphaericus (BS) are microbial larvicides that
occur naturally in soils and aquatic environments
globally. The active ingredients of Bti formulations are
delta-endotoxin crystals produced by various species of
bacteria. Mosquito larvae eat the Bti product that is
made up of the dormant spore form of the bacterium
and an associated pure toxin. The toxin disrupts the gut
in the mosquito by binding to receptor cells present in
insects, but not in mammals. Bti is registered as a
pesticide for control of mosquito larvae in outdoor
areas such as irrigation ditches, flood water, standing
ponds, woodland pools, pastures, tidal water, fresh or
saltwater marshes, and storm water retention areas.
Extensive testing shows that Bti does not pose risks to
wildlife, non-target species, or the environment, when
used according to label directions.
Bacillus sphaericus is another bacterial
larvicide that occurs naturally and is found throughout
the world. BS acts in a manner similar to Bti. The
bacteria are ingested by the mosquito larvae and the
toxin disrupts the gut in the mosquito by binding to
receptor cells present in insects but not in mammals. BS
toxins are much slower acting than Bti toxins but their
effectiveness is more persistent. Both Bti and BS are
classified as Biopesticides by EPA and both bear the
“CAUTION” signal word in their product labels.
26
Adulticides
Currently, two classes of pesticides are widely
used for the majority of adulticiding operations in
Florida. These are the organophosphates (OP) and
pyrethroids. The OP used in Florida includes malathion,
naled and chlorpyrifos. The pyrethroids consist of
pyrethrum, pyrethrins, permethrin, resmethrin,
lambda-cyhalothrin, cyfluthrin and D-phenothrin.
Etofenprox, a pyrethroid-like compound, was recently
registered and has been used to a small extent.
Malathion is an organophosphate (OP)
insecticide that has been registered for use in the
United States since 1956. Malathion kills mosquitoes
because it is converted inside the mosquito into mala-
oxon, which inhibits an important central nervous
system enzyme called acetylcholinesterase (AChE).
AChE breaks down the neurotransmitter, acetylcholine.
When this enzyme is inhibited by an OP, the
neurotransmission cannot cease and the nerve is over
stimulated. Ultimately, this overstimulation leads to
paralysis and death in the mosquito. All
organophosphate insecticides share this mode of action.
Malathion can be applied using both ground
and aerial equipment to control adult mosquitoes.
Malathion is a very effective chemical control agent and
when applied in accordance with the label
recommended rate and safety precautions, this
compound poses no unacceptable risks to human health
or the environment.
Naled is also an OP pesticide that is primarily
used for aerial adulticiding in Florida. It has a similar
mode of action again adult mosquito to malathion.
Naled is highly toxic to insects, and therefore is typically
applied at less than an ounce per acre. Like malathion,
the risks from naled to humans, birds, and fish are not
unacceptable. However, because of the invertebrate
toxicity of this compound, there are risks to non-target
invertebrates, including beneficial insects such as
honeybees. For that reason, EPA has established specific
precautions on the label to reduce such risk.
Pyrethrins are naturally-occurring
compounds derived from members of the
chrysanthemum family. Pyrethrins act on sodium
channels through which sodium is pumped to cause
excitation and nerve transmission. They prevent the
sodium channels from closing, resulting in continual
nerve impulse transmission, tremors, and eventually,
muscle paralysis and death. Since they are naturally
occurring compounds and break down rapidly in
sunlight, they are considered as environment-friendly
adulticides and have few negative residual effects.
Pyrethroids are synthetic chemical
insecticides whose structures mimic the natural
insecticide pyrethrum. Permethrin, resmethrin, and
sumithrin are synthetic pyrethroids commonly used in
Florida to control adult mosquitoes. Pyrethroids, like
pyrethrins, kill insects by overexciting their nervous
system. When used appropriately, pyrethroids used in

mosquito control programs should not pose
unreasonable risks to wildlife or the environment.
Pyrethroids, when applied at mosquito control rates,
are low in toxicity to mammals, and are practically non-
toxic to birds. However, pyrethroids are toxic to fish and
to bees. For that reason, EPA has established specific
precautions on the label to reduce such risks, including
restrictions that prohibit the direct application of
products to open water or within 100 feet of lakes,
streams, rivers or bays.
Other Control Methods
The Department of Agriculture and Consumer
Services has for many years stressed the importance of
permanent control, but because chemical insecticides
have been questioned by environmentalists in recent
years, additional emphasis has been put on research to
find alternative methods of controlling mosquitoes.
Biological control of a population through an increase in
predators or pathogens affecting the organism to be
controlled has been practiced in mosquito control for
many years. For instance, digging minnow-access
ditches into a salt marsh or stocking mosquito breeding
areas with fish, which feed on larvae are two such
means to control mosquitoes. However, opposition by
special interest groups and recently enacted legislation
restricting the construction of ditches, have all but
eliminated this biological control method for mosquito
control.
Researchers are also continuing to study
bacterial, protozoan, fungal, algal, and viral diseases of
mosquito larvae. It is hoped that a number of effective
biological control agents may be discovered from these
efforts.
Mosquito control programs may also apply
herbicides to kill aquatic weeds that provide protection
and, in certain species, oxygen for the larvae. Research
is also underway to determine the feasibility of using
the sterile male technique to control mosquito
populations. At the Florida Medical Entomology
Laboratory, researchers are studying lethal genes as a
hope for genetic control. But at the present time, none
of these methods are available and effective in practical
control operations.
Whatever methods of control may be used by
a district, it is of the utmost importance that they be
chosen carefully and used with utmost safety. This is
especially true in the use of chemical insecticides. Only
materials labeled for that particular use can be utilized.
These products should also be applied at the lowest
effective concentration, in strict accordance with the
label. The equipment used to apply the insecticide
should be properly calibrated and carefully checked,
and the applicator should be fully trained in the safe
handling and application of the material used. The
importance of using chemicals in the recommended
manner (i.e. proper rate, correct vehicle speed and
swath width) so that it is safe both to the environment
and to the applicator cannot be overemphasized.
Insecticides should be used only when absolutely
necessary and never on a routine basis.
Integrated Mosquito Management (IMM)
The most effective programs in mosquito
control are based on a combination of methods. These
include water/habitat management, chemical control
and biological control. This multi-tooled approach is
called "integrated control." To use integrated control
effectively, it is necessary to have a broad
understanding of the insects to be controlled and the
factors which influence population size. In this way,
costly chemical controls can be used only when really
needed and when they will be most effective.
In 2009, the American Mosquito Control
Association (AMCA) drafted a new policy document on
Integrated Mosquito Management (IMM). This
document was made available to EPA to help guide its
deliberations regarding National Pollutant Discharge
Elimination System (NPDES) permits. This document is
also discusses Best Management Practices (BMP) that,
when practiced by mosquito control agencies, will serve
as a basis for developing an Integrated Mosquito
Management (IMM) approach to mosquito control in
Florida. IMM is the use of a combination of biological,
chemical, educational and physical control methods in
order to maintain targeted mosquito species or
populations of mosquitoes at acceptable levels.
Legal Aspects of Mosquito Control
Mosquito control districts and programs are
established and operated under the authority provided
in the Mosquito Control Law, Chapter 388 Florida
Statutes (F. S .), and the Mosquito Control Rules,
Chapter 5E-13, Florida Administrative Code (F.A.C.).
Chapter 388 F.S. provides local governmental entities
authority to conduct arthropod control on public land,
under conditions specified in the law.
Performance of control measures on private
property requires permission of the owner. In cases
where the owner will not control arthropod breeding
on his property and refuses to permit the mosquito
control district to do so, it may be necessary to use the
authority provided in Chapter 386 F.S., Particular
Conditions Affecting Public Health. District Directors
are encouraged to work with the local Department of
Health officials and the homeowner to amicably resolve
and minimize potential health threats.
The Federal Insecticide, Fungicide, and
Rodenticide Act of 1972 requires that the EPA be
certain that all personnel handling hazardous or
restricted chemicals be trained to do so correctly and
safely, and that they be certified as pesticide applicators
by a responsible state or federal agency.
27

The state agency to administer the
certification is appointed by the governor of each state.
In Florida, the Department of Agriculture and Consumer
Services has been designated as the lead agency, and
shall be responsible for certifying the commercial pest
control operators and mosquito control personnel
making pesticide applications in the State. The law
requires that every person applying pesticides for
mosquito control, with certain exemptions, be certified
or be supervised by a certified applicator.
A mosquito control director is responsible for
upholding a number of laws and regulations related to
the safe use of pesticides and application equipment by
program employees. The director should ensure that all
applicators read and understand pesticide labels, that
they wear and maintain appropriate personal
protective equipment (PPE), that they follow the
recommended procedures in storing and mixing
chemicals, and in disposing of empty containers, that
they are well trained in proper operation of equipment,
and that they know and use good driving habits.
The director is also responsible for securing
adequate insurance for the district, and meeting the
requirements of the Social Security Act, "Right to Know"
law, and the Occupational Safety and Health Act (OSHA).
Public Relations and Dealing with Negative Impacts
To build a really effective mosquito control
program the general public must be made aware of the
need for mosquito control, the methods by which it is
accomplished, and the need for their support and
cooperation. How well a program is explained to the
public will determine not only the amount of tax money
the program receives, but the cooperation received
from land owners on whose property it is necessary to
work. It will influence the concern and cooperation
citizens give in trying to keep their premises free of
receptacles which might breed mosquitoes.
The public image of a mosquito control district
is created in three ways -through public coverage such
as newspaper stories and radio and television
announcements and programs, by talking before civic
organizations, schools and other groups, and by dealing
with individuals through telephone calls, letters or
personal contact.
The word "relations" in public relations
indicates that a relationship should exist and that the
process involves an exchange of information to and
from the public. Telephone calls and letters from the
public give the director an indication of where the
mosquitoes may be present at nuisance or public health
concern levels, how the public is reacting to the control
measures being used, and what the public wants done
that is not being done. This is invaluable information
and the director should follow-up complaints with
either an inspection or surveillance. In addition, every
employee of the district should be aware that the image
they create as they go about their job determines how
the public feels about mosquito control. Courtesy and
safety in driving, patience and consideration in dealing
with questions and problems, and care when working
on other people's property will give the public a
favorable view of the program.
Wherever a large scale mosquito control
program operates some negative impacts, both real and
perceived, will occur. Groups that occasionally oppose
some or all mosquito control activities include
environmental organizations, beekeepers, public lands
managers, aquaculturists, organic farmers, concerned
citizens, and chemically sensitive or chronically ill
individuals.
A mosquito control director has a
responsibility to work with these groups to achieve a
compromise acceptable to all concerned. The first step
is opening the lines of communication and to
developing trust. Often, the main problem is a lack of
understanding on both sides. Through education the
concerned party may better understand the need for,
and minimal impact of control operations and the
mosquito control director may realize how small
changes in the operation may significantly decrease the
possibility of adverse effects. Beekeeping is a good
example. Honey bees are susceptible to
organophosphates such as the adulticides naled,
chlorpyrifos, and malathion, and the larvicide
temephos. As a result, adulticiding during times of high
bee activity and larviciding over bee yards may have an
impact on the honey bee populations. Most aerial
adulticiding is now performed early in the morning
before bees leave the hive to forage, or in the evening or
at night when bees are back in the hives, thus
minimizing any impacts. In addition, mosquito control
personnel advise local beekeepers as to which areas will
have high, low, or no aerial activity allowing them to
locate their bee yards in "safe" areas. Beekeepers are
encouraged to inform mosquito control when they plan
to move their hives. If mosquito control is aware of bee
yards in or close to areas regularly treated, they can
tailor the operations to avoid impacts on the bees, such
as switching larvicides from temephos to a safer
material, such as methoprene or Bti.
Many mosquito control programs maintain a
listing of concerned citizens. Often these individuals
understand the need for mosquito control operations
but are fearful of exposure to any chemicals, despite
education and assurances from scientific experts. In
most cases, the solution to this problem is simple: the
district can call the concerned citizen(s) to inform them
of upcoming spray operations in their area. The citizen
can then take whatever precautions they deem
necessary to avoid exposure, and they feel mosquito
control has made an effort to work with them.
28

Arthropods of Public Health Importance
Mosquito control directors will often be asked
to identify, provide advice and possibly help in
controlling arthropods other than mosquitoes. Usually,
the questions relate to insects which bite or sting, but it
is not uncommon to receive questions about arthropods
which are annoying because of their abundance.
Among the insects which are frequently
reported as annoying are the blind mosquitoes
(Chironomidae) which may emerge from lakes of
Florida in such huge numbers that they make outdoor
living impossible and may even be a traffic hazard.
These insects are very similar to mosquitoes in
appearance, but they do not have scales on the wings
and the adults do not feed on blood. When very large
populations of these insects occur, it would be virtually
impossible for an individual to control these insects. A
mosquito control district can, however, cover a large
enough area with adulticides to give temporary relief.
The lovebugs (Bibionidae) are another major
annoyance in Florida. They fly into roadways in such
large numbers during peak emergences that
windshields are quickly covered with spattered insects.
The worst period is usually April through May, with a
secondary occurrence in September. Inside homes there
are sometimes populations of booklice (Psocidae) large
enough to create an annoyance by crawling on the skin.
These insects are not true lice and do not bite.
A number of people have entomophobia, a fear
of insects, and “suffer” from bites and crawling insects
on the skin which are often imagined rather than real.
Certain insects and arachnids are feared
because they can give a painful bite or sting. Those
which inject venom by biting include the black widow
spider, the brown recluse spider (not usually found in
Florida) and certain ticks. Those which inject venom by
stinging include scorpions, wasps, bees and fire ants.
The venom produces irritation at and around the site of
the injection. When the person is allergic to the venom,
more severe reactions may result including
anaphylactic shock and even death.
The urticating caterpillars inject their venom
through hollow body hairs. When a person brushes
against the hairs, venom passes from blades at the base
of the hair into the skin of the individual, producing a
very painful sting. The puss moth caterpillar,
saddleback, and IO moth caterpillar are the most
commonly encountered stinging caterpillars.
There also are a number of insects which shed
wing scales or hairs that may cause allergic reactions in
some individuals. Symptoms include itching and
dermatitis in sensitive individuals. The mouthparts of
many insects such as bedbugs, lice, some flies, mites and
ticks are constructed for blood sucking and in many
instances a blood meal is required for the female before
eggs can be developed and laid.
Dog flies (a.k.a., stable flies), sand flies, horse
or deer flies, fleas, chiggers and bird mites do not inject
venom when biting, but their saliva may be very
irritating or painful. Most of these insects do not usually
transmit diseases.
The larvae from a few fly species have been
known to survive internally in man, but these cases are
usually the result of accidental infestation and occur
infrequently. However, both flies and the screw worm
may lay their eggs in wounds or in the nostrils of man,
and the maggots can cause a very serious health
problem if not promptly treated by a skilled physician.
The role of mosquitoes in disease
transmission has been previously discussed. However, a
number of other insects are also involved in the spread
of human diseases.
Some examples of mechanical or passive
transmission of diseases would include the spreading of
"pink eye" or conjunctivitis by eye gnats, the spread of
typhoid and intestinal diseases by house flies and the
potential spread of pathogenic and food poisoning
organisms by cockroaches.
Aside from mosquitoes, the arthropod vectors
of diseases most likely to be encountered in Florida are
ticks and fleas. Although endemic typhus, spread by rat
fleas, was once widespread in the State, it is no longer a
concern here.
Rocky Mountain spotted fever, Lyme disease,
human ehrlichioses and tularemia are human diseases
which are vectored by ticks. The usual vector of Rocky
Mountain spotted fever, the American dog tick,
Dermacentor variabilis, occurs in Florida, but the
disease itself is almost unheard of in the State. Lyme
disease is caused by a spirochete and is found primarily
in the northeast and pacific coast areas of the U.S. The
disease is vectored by Ixodid ticks. The human
ehrlichioses are a complex of tick-borne rickettsial
diseases that are generally mild but may become
serious if not treated early. Cases of tuleremia do occur,
but in Florida most of these have been traced to dermal
contact with infected rabbits, and not tick bites.
A few cases of tick paralysis have been
recorded in Florida, usually in children who were found
to have one or more ticks attached near the hairline on
the neck. Careful removal of the ticks has been followed
by a swift recovery from the paralysis.
Mosquito Control directors should learn to
recognize the more common of these annoying or
dangerous arthropods, and should be able to provide
information on their life histories and control when
requested. The Florida Insect Control Guide will be
especially useful for this purpose.
29

Control of Other Arthropods by Mosquito Control Districts
In instances where insects other than
mosquitoes breed in such numbers as to be a serious
nuisance or a health hazard to the public, the mosquito
control district will often be called on to control these
insects or other arthropods. The most frequent
problems encountered are sand flies, dog flies, midges
(blind mosquitoes), house flies and other filth flies, and
eye gnats.
Sand Flies (Figure 26). - These small
biting midges of the genus Culicoides are a pest in many
areas of Florida, although the coastal species cause
more annoyance than the freshwater species. Much
research has been directed toward finding methods and
materials to effectively control these pests, but with the
exception of water management, no really satisfactory
method has been found. The only solution is to keep
their breeding areas flooded completely, or to fill them
and construct bulkheads at the shoreline.
Several chemical insecticides can be very
effective in killing sand fly larvae, but some of these
materials are also highly toxic to the aquatic fauna and
other wildlife. Panasol, a petroleum solvent, can be used
effectively as a larvicide and with safety to non-target
species; but because of the large volume required for
coverage, this larvicide is practical only for treating
shorelines. Research is being conducted with IGR
compounds, and they are showing promise as larvicides
for sand flies.
When sand fly adults are a problem in
populated areas, it is possible to fog or spray and
control them, but new adults move in from the
periphery so rapidly that relief is very temporary. In
addition, the results often do not justify the cost. Unless
the problem can be resolved by impounding or filling
the breeding area, the only real solution at the present
time is for people to try to remain inside air-
conditioned buildings when populations are high. If the
flies get indoors, household aerosols will provide
control. Repellents offer some protection for several
hours when one must be outside, but do not repel these
insects as well as they do mosquitoes. Fortunately,
these insects are seasonal in nature.
Stable Flies (Figure 27). - Also known as
dog flies, stable flies are a major pest along the
northwest Gulf coast from Wakulla County through
Escambia. The flies have a known flight range of up to
70 miles. In the past, the State had a modest
appropriation to carry out control operations which
would supplement the control operations of the
counties. Counties in the stable fly area should have
organized inspection and surveillance protocols for
stable fly outbreaks. Beaches must be inspected daily
for adult flies, starting at 8:00 a.m. and at least once or
twice more during the day, as long as north winds
prevail. Stable fly larvae should be controlled where
possible by management of plant and animal wastes to
destroy the larvae without the use of sprays. This can be
done by spreading waste materials thinly at intervals so
that they dry quickly.
Figure 26. Sand Fly
Figure 27. Stable Fly
30

Blind Mosquitoes (Chironomidae)
(Figure 28). - These mosquito-like insects do not bite,
nor carry disease. However, they are a nuisance when
they emerge in such large numbers that they make
outdoor activities unpleasant or impossible. Blind
mosquitoes have also been known to come to homes in
such huge numbers, attracted by the lights, that they
enter every time a door is opened.
Most complaints about midges come from the
lake regions in Polk, Orange, Lake, Highlands, and
Seminole counties, from sites along the St. Johns River
or its tributaries, or from the vicinity of man-made lakes
at apartment or condominium sites. Organic pollution,
including sewage treatment effluents, canning wastes
and fertilizer carried off by ground water, is responsible
for the heavy production.
In the past there have been several programs
for control of midge larvae with various insecticides. At
present, most efforts are directed toward control of
adult midges.
House Flies (Figure 29). - House flies and
other filth flies are capable of breeding in almost any
warm, moist organic matter such as animal manure,
garbage, or decomposing foods. Control of house flies
and other filth flies is usually best accomplished by
good sanitation, and the arthropod control districts are
called in only when an unusual situation causes a
problem population -such as an improperly managed
landfill. House flies have developed resistance to many
of the chlorinated hydrocarbon and organophosphate
insecticides. It is best to consult the most recent
recommendations for control before treating for flies.
Eye Gnats (Figure 30). - Until the last
decade, eye gnats were only a localized and temporary
problem in the State. However, with conversion of vast
tracts of woodlands in west Florida into farms for
growing soybeans and other crops, eye gnats have
become a significant problem. With eye gnats, as with
many problem insects, adulticiding offers, at best,
temporary relief. Newly emerged adults quickly reinfest
the sprayed areas. IGR compounds have shown promise
in current research for control of the larval stage.
Miscellaneous Insects. Mosquito control
districts often receive calls from private citizens seeking
information on how to control other certain household
pests, such as fleas, roaches, ticks, etc. Although
controlling these types of pests may not fall under the
mission of the program it is a good public relations step
to have the information at hand to give them. The
Florida Cooperative Extension Service, University of
Florida’s website
(http://edis.ifas.ufl.edu/topic_guide_ig_household_pests
_and_pests_of_man), is an excellent source of up-to-date
information on control.
Figure 28. Blind mosquito life cycle
Figure 29. House Fly
Figure 30. Eye Gnat
31

GLOSSARY
Arbovirus: Arthropod-borne viral disease agent transmitted biologically by insects.
Arthropod: An animal of the phylum Arthropoda characterized by having a hard exoskeleton, body with a number of
segments arranged longitudinally and paired jointed appendages. The phylum Arthropoda includes insects, spiders,
mites, ticks, scorpions, centipedes, millipedes, etc.
Calibration: The adjustment of pesticide application equipment to apply a pesticide formulation at a desired application
rate.
Cuticle: Thin, multilayered tissue covering insects and other arthropods. The outside layer is composed of proteins,
waxes and “cement”, while layers beneath contain chitin along with proteins and waxes penetrated by numerous pores
and glands.
DACS: Florida Department of Agriculture and Consumer Services.
Ditching: Creating ditches or furrows into a salt marsh to provide water circulation and to make the marsh available to
fish.
Eastern Equine Encephalitis (EEE): Eastern equine encephalitis is a viral disease that is spread to horses and humans
by infected mosquitoes. The causative agent, eastern equine encephalitis virus (EEEV), is an alphavirus that was first
isolated from infected horse brains in 1930s and currently occurs in focal locations of the eastern United States including
Florida
Enzootic: Animal diseases which are commonly present in a locality.
Exoskeleton: The hard or tough external covering of arthropods to which their muscles are attached and which serves
the same function as the bony skeleton of humans.
FAMA: Florida Anti-Mosquito Association.
Family: A group of related genera within an order.
Fauna: Animal life of a given area.
Faunal Zones: is a generic term for the list of animal species occurring in a particular region. Fauna can refer to a
prehistoric collection of animals, as might be inferred from the fossil record, or to a modern assemblage of species living
in a region. More locally, a faunation refers to the communities of individuals of the various animal species and occurring
in a particular place.
Flora: Plant life of a given area.
FMCA: Florida Mosquito Control Association.
FMEL: Florida Medical Entomology Laboratory, University of Florida, Institute of Food and Agricultural Sciences.
Genus (genera): A group of species considered more closely related to one another than to members of another genus
(plural is “genera”); the first word in the scientific name of a species is the name of the genus.
Impoundment: Coverage of the surface of a marsh with shallow water to prevent exposing substrate for salt march
mosquito egg laying.
Insect Growth Regulator (IGR): Synthetic insecticide which prevents normal development or causes delayed mortality
of insects by disrupting a natural physiological process.
Integrated Mosquito Management (IMM): The use of a combination of biological, chemical, educational and physical
control methods in order to maintain targeted species or populations of mosquitoes at an acceptable level.
32

Label: General and technical information about a pesticide product in the form of printed material attached to or printed
on the pesticide container.
Labeling: Technical information about a pesticide in the form of printed material provided by the manufacturer,
including labels, flyers, handouts, leaflets and brochures.
Landing Rate Count: A method of determining adult mosquito levels by counting all mosquitoes that land on the visible
portion of the body during a one minute period. Results are expressed as numbers of mosquitoes per minute.
Mosquito Control Law: Chapter 388 Florida Statutes (F. S.) makes provision for arthropod control to be conducted on
public land with certain conditions to be met.
Mosquito Control Rules: Chapter 5E-13, Florida Administration Code (F.A.C) to spell out mosquito control law.
Palpus (pl. palpi): Five-segmented paired sensory appendages projecting from the base of the proboscis.
PHEREC: The John A. Mulrennan, Sr. Public Health Entomology Research and Education Center, Florida A & M University.
PPE: Personal protective equipment.
Proboscis: Extended mouth structure of insects; the piercing mouth parts of a female mosquito which is made up of a
sheath-like structure (labium) enclosing piercing and sucking structures.
Seepage: Movement of water through the soil to form a pool on the surface.
St. Louis Encephalitis (SLE): Arboviral infection normally maintained in rural or urban areas as an enzootic cycle among
wild birds by Culex mosquito vectors. During mid to late summer, viral levels in the wild bird populations may be high
enough for transmission to humans by the same vector species.
Subfamilies: A taxonomic category of related organisms ranking between a family and a genus.
Tarsus (tarsi): The last segments of an insect’s legs; the “feet” of an insect (plural is tarsi).
Ultra-low volume (ULV): A spray application of a pesticide that is a technical or undiluted material and broken up into
very small droplets.
West Nile Virus (WNV): A flavivirus that is transmitted by mosquitoes.
33

Bibliography
Additional References on Mosquito Control and Mosquito Identification
1960. King, W. V., G. H. Bradley, C. N. Smith and W. C. McDuffie. Mosquitoes of the Southeastern United States.
Agriculture Handbook No. 173. Agricultural Research Service, USDA. 188 pp.
1968. American Mosquito Control Association. Ground Equipment and Insecticides for Mosquito Control. Bulletin No. 2.
1970. American Mosquito Control Association. Manual for Mosquito Rearing and Experimental Techniques. Bulletin No.
5.
1977. U.S. Dept of Health, Education and Welfare. Mosquitoes of Public Health Importance and Their Control. (Revised)
HEW Publ. No. (CDC) 77-8140. U.S. Public Health Service C.D.C., Atlanta, GA 55 pp.
1982. American Mosquito Control Association. The Use of Aircraft for Mosquito Control. Bulletin No. 1. Revised.
1982. Breeland, S. G., and T. M. Loyless. Illustrated Keys to the Mosquitoes of Florida: Adult Females and Fourth Stage
Larvae. Journal of Florida Anti-Mosquito Assocation. 53(2): 63-84.
1983. Breeland, S. G., and J. A. Mulrennan, Jr. An Overview of Organized Mosquito Control in Florida. Mosquito News.
47(3): 276-280.
2000. Darsie, R. H. and C. D. Morris. Keys to the Adult Females and Fourth Instar Larvae of the Mosquitoes of Florida.
Bulletin of the Florida Mosquito Control Association, No. 1. (revised) 159 pp.
2004. Florida Mosquito Control Association. H. T. Evans' Florida Mosquito Control Handbook. Ed.: Rutledge C. R.
2004. Darsie, R. F., Jr., and R. A. Ward. Identification and Geographical Distribution of the Mosquitoes of North America,
North of Mexico. University Press of Florida.
2009. Florida Coordinating Council on Mosquito Control. Florida Mosquito Control (“White Paper”). Connelly C. R. and D.
B. Carlson, Co-Chairs, Steering Committee.
34
